
Key findings from a study about intergenerational caregiving experiences of Canadian Chinese immigrant mothers
Topic: Mothers
Report: Fertility Treatment in Canada
An overview of fertility treatments, policies, and provincial subsidies available in Canada
Then and Now: A 30-Year Look at Families and Work in Canada
Highlights from a resource about families and work in Canada
Report: Mothers’ Return to Work After Childbirth and the Role of Spousal Involvement at Home

A report on the impacts of mothers’ return to work after childbirth on their mental wellbeing
Amy Robichaud

Amy is the daughter to Lore, granddaughter to Rae, and great granddaughter to Rita.
She currently serves as CEO at Mothers Matter Canada and previously as Executive Director of Dress for Success Vancouver, Director of Engagement at the Minerva Foundation for BC Women, and as a development and governance consultant to organizations such as the RBC Foundation, the Global Centre for Pluralism, and the Canadian Mental Health Association.
Amy’s passion for practical ways to generate equity, create economic inclusion, opportunity and prosperity for all informs everything she does, including her volunteerism. She is serving her second term as Chair of the Women’s Advisory Committee for the City of Vancouver where she advises Council and staff on enhancing access and inclusion for women and girls to fully participate in City services and civic life. She has previously served as Chair of the Dress for Success Canada Foundation, and was nominated for the YWCA Vancouver’s Women of Distinction Awards in 2023. She’s a member of the Banff Forum and WNORTH.
Amy and her husband have lived all over Canada and now happily and humbly call the unceded, ancestral and traditional territories of the xʷməθkʷəy̓əm, Sḵwx̱wú7mesh, and səlilwətaɬ Nations home, along with their pets and overgrown library.
About Mothers Matter Canada
Mothers Matter Canada (MMC) is a national organization dedicated to empowering socially isolated and economically vulnerable mothers by providing innovative, evidence-based programs that support early childhood education, strengthen parent-child bonds, and promote community integration. Through partnerships and advocacy, MMC works to break cycles of poverty and isolation, ensuring mothers and their children achieve their full potential and thrive in welcoming, inclusive communities. When mothers thrive, children flourish, and communities prosper.
Margaret Campbell

Margaret Campbell received her PhD in Social and Cultural Analysis from Concordia University. Her thesis, which was supported by a grant from the Social Sciences and Humanities Research Council of Canada (SSHRC), explored the diverse ways that people with disabilities make sense of their sexual health and expression. Her PhD research examined barriers to sexual health and expression that many persons with disabilities face and identified diverse ways that they create opportunities for sexual expression despite these barriers. As a post-doctoral fellow with the Vanier Institute, Margaret conducted research aimed at strengthening our understanding of family diversities and family wellbeing, specifically among families with disabilities.
Margaret’s research interests in the wellbeing of families with disabilities and families of those who work in high-risk occupations stem from her upbringing on a family farm in rural Prince Edward Island and her personal experience living with a chronic illness.
Margaret teaches on a part-time basis at St. Thomas University and has a breadth of experience teaching courses in Family Studies, Sociology, and Gender Studies. Her teaching and research practices are informed by critical theories, feminist frameworks, and her belief in the possibility of creating a world that is more equitable, accessible, and, ultimately, more livable.
Robin McMillan

Robin McMillan has spent her career of over 30 years working in the early learning sector. For the first eight years, she worked as an Early Childhood Educator with preschool children. She left the front line to develop resources for practitioners at the Canadian Child Care Federation (CCCF). She has been with the CCCF since 1999 and worked her way from Project Assistant to Project Manager to her present role as Innovator of Projects, Programs and Partnerships. Highlights of her career with CCCF have been managing over 20 national and international projects, including a CIDA project in Argentina and presenting a paper with the Honourable Senator Landon Pearson to the Committee on the Rights of the Child in Geneva, Switzerland.
Robin served as a board member on the Ottawa Carleton Ultimate Association for two years, as well as participated in organizing numerous local charity events. She founded and facilitated a local parent support group, Ottawa Parents of Children with Apraxia, and a national group, Apraxia Kids Canada. She is married and has a 17-year-old son with a severe speech disorder, childhood apraxia of speech, and a mild intellectual disability, which launched her into the world of parent advocacy. She was the recipient of the Advocate of the Year Award in 2010 from the Childhood Apraxia of Speech Association of North America.
About the Organization: We are the community in the early learning and child care sector in Canada. Professionals and practitioners from coast to coast to coast belong in our community. We give voice to the deep passion, experience, and practice of Early Learning and Child Care (ELCC) in Canada. We give space to excellent research in policy and practice to better inform service development and delivery. We provide leadership on issues that impact our sector because we know we are making a difference in the lives of young children—our true purpose, why we exist—to make a difference in these lives. What gets talked about, explored, and shared in our community is always life changing, and we know that. We are a committed, passionate force for positive change where it matters most—with children.
Maude Pugliese

Maude Pugliese is an Associate Professor at the Institut national de la recherche scientifique (Université du Québec) in the Population Studies program and holds the Canada Research Chair in Family Financial Experiences and Wealth Inequality. She is also the scientific director of the Partenariat de recherche Familles en mouvance, which brings together dozens of researchers and practitioners to study the transformations of families and their repercussions in Quebec. In addition, she is the director of Observatoire des réalités familiales du Québec/Famili@, a knowledge mobilization organization that diffuses the most recent research on family issues in Quebec to a broad public in accessible terms. Her current research work focuses on the intergenerational transmission of wealth and of money management practices, gender inequalities in wealth and indebtedness, and how new intimate regimes (separation, repartnering, living apart together, polyamory, etc.) are transforming ideals and practices of wealth accumulation.
Gaëlle Simard-Duplain

Gaëlle Simard-Duplain is an Assistant Professor in the Department of Economics at Carleton University. Her research focuses on the determination of health and labour market outcomes. She is particularly interested in the interaction of policy and family in mitigating or exacerbating inequalities, through both intrahousehold family dynamics and intergenerational transmission mechanisms. Her work predominantly uses administrative data sources, sometimes linked to survey data, and quasi-experimental research methods. Gaëlle holds a PhD in Economics from the University of British Columbia.
Donna S. Lero

Donna S. Lero is University Professor Emerita and the inaugural Jarislowsky Chair in Families and Work at the University of Guelph, where she co-founded the Centre for Families, Work and Well-Being. Donna does research in Social Policy, Work and Family, and Caregiving. Her current projects focus on maternal employment and child care arrangements, parental leave policy, and disability and employment, as well as the Inclusive Early Childhood Service System (IECSS) project and the SSHRC project Reimagining Care/Work Policies.
Barbara Neis

Barbara Neis (PhD, C.M., F.R.S.C.) is John Lewis Paton Distinguished University Professor and Honorary Research Professor, retired from Memorial University’s Department of Sociology. Barbara received her PhD in Sociology from the University of Toronto in 1988. Her research focuses broadly on interactions between work, environment, health, families, and communities in marine and coastal contexts. She is the former co-founder and co-director of Memorial University’s SafetyNet Centre for Occupational Health and Safety and former President of the Canadian Association for Work and Health. Since the 1990s, she has carried out, supervised, and supported extensive collaborative research with industry in the Newfoundland and Labrador fisheries including in the areas of fishermen’s knowledge, science, and management; occupational health and safety; rebuilding collapsed fisheries; and gender and fisheries. Between 2012 and 2023, she directed the SSHRC-funded On the Move Partnership (www.onthemovepartnership.ca), a large, multidisciplinary research program exploring the dynamics of extended/complex employment-related geographical mobility in the Canadian context, including its impact on workers and their families, employers, and communities.
Deborah Norris

Holding graduate degrees in Family Science, Deborah Norris is a professor in the Department of Family Studies and Gerontology at Mount Saint Vincent University. An abiding interest in the interdependence between work and family life led to Deborah’s early involvement in developing family life education programs at the Military Family Resource Centre (MFRC) located at the Canadian Forces Base (CFB) Halifax. Insights gained through conversation with program participants were the sparks that ignited a long-standing commitment to learning more about the lives of military-connected family members—her research focus over the course of her career to date. Informed by ecological theory and critical theory, Deborah’s research program is applied, collaborative, and interdisciplinary. She has facilitated studies focusing on resilience(y) in military and veteran families; work-life balance in military families; the bi-directional relationship between operational stress injuries and the mental health and wellbeing of veteran families; family psychoeducation programs for military and veteran families; and the military to civilian transition. She has collaborated with fellow academic researchers, Department of National Defense (DND) scientists, Veterans Affairs Canada (VAC) personnel, and others. Recently, her research program has expanded to include an emphasis on the impacts of operational stress on the families of public safety personnel.
Diane-Gabrielle Tremblay

Diane-Gabrielle Tremblay is professor of labour economics/sociology and human resources management at TÉLUQ University (Université du Québec). She was appointed Canada Research Chair on the socio-economic challenges of the Knowledge Economy in 2002 and director of a CURA (Community-University Research Alliance) on the management of social times and work-life balance in 2009 (www.teluq.ca/aruc-gats). She is a Fellow of the Royal Society of Canada and of the Centre of Excellence of the Université du Québec, in recognition of the quality of her research and publications. She works on work-life issues, work organization (telework, coworking), and working time arrangements. Diane-Gabrielle has published many books, including a Labour Economics textbook, a Sociology of Work textbook, three books on working time and work-life issues and she has published in various international journals.
Shelley Clark

Shelley Clark, James McGill Professor of Sociology, is a demographer whose research focuses on gender, health, family dynamics, and life course transitions. After receiving her PhD from Princeton University in 1999, Shelley served as program associate at the Population Council in New York (1999–2002) and as an Assistant Professor at the Harris School of Public Policy at the University of Chicago (2002–2006). In the summer of 2006, she joined the Department of Sociology at McGill, where in 2012 she became the founding Director of the Centre on Population Dynamics. Much of her research over two decades has examined how adolescents in sub-Saharan Africa make key transitions to adulthood amid an ongoing HIV/AIDS epidemic. Additional work has highlighted the social, economic, and health vulnerabilities of single mothers and their children in sub-Saharan Africa. Recently she has embarked on a new research agenda to assess rural and urban inequalities and family dynamics in the United States and Canada. Her findings highlight the diversity of family structures in rural areas and the implications of limited access to contraception on rural women’s fertility and reproductive health.
Lindsey McKay

Lindsey McKay is an Assistant Professor in Sociology at Thompson Rivers University in Kamloops, British Columbia. She is a feminist sociologist/political economist of care work, health and medicine, and the Scholarship of Teaching and Learning. Social justice motivates her research and teaching. She has published in peer-reviewed journals and public platforms on parental leave inequity, organ donation, and curriculum and pedagogy. She is a Co-Investigator in the SSHRC funded Reimagining Care/Work Policies project with a focus on parental leave.
Research Snapshot: Mothers and Part-time Work: Preferences and Experiences
Families Count 2024: Family Structure

Family Structure is the first section of a larger report that will also explore family work, family identity, and family wellbeing.
Research Snapshot: Inuit Mothers’ Visions for Child and Family Wellness in Nunavut, Canada

Summary of a study on how the child welfare system is perceived by Inuit mothers
Research Snapshot: Overwork, Remote Work, and Gendered Dual Devotion to Work and Family

Summary of a study on how dual devotion differs based on gender
Research Snapshot: Challenges of Non-Standard Work Schedules and Childcare

Summary of a study on the unique challenges of managing non-standard work hours and childcare
Research Snapshot: Gaps in Employment Protections for Pregnant Migrants in Canada

Summary of a study on women who were pregnant or gave birth while having precarious immigration status
Research Snapshot: “Family Stories” and Intergenerational Voices of Adoption

A summary of a study on the effects of adoption in adulthood
Research Snapshot: Maternal Labour Force Participation and Separation Anxiety Among Children

Findings from a study about working mothers and separation anxiety among children
Fertility Rate in Canada Fell to (Another) Record Low in 2022
New data shows Canada’s fertility rate is at (another) new record low.
Research Snapshot: Parents, Homeschooling, and Relationship Conflict During COVID-19

Highlights from a study on how providing homeschooling during COVID affected parents
Research Snapshot: Examining Benefits and Barriers to Participating in Family Physical Activity

Highlights from a study about families and active leisure
Three Takeaways from the Quebec Childcare Model

Lessons from Quebec’s childcare system for other provinces and territories in Canada
Research Snapshot: Parenthood and the Gendered Impact of Job Loss
Highlights from a study about gendered consequences of job loss
Policy Brief: Access to Parental Benefits in Canada
A 50-year review of access to parental benefits in Canada
Research Snapshot: Factors Influencing Parents’ Work-Life Balance Inside and Outside Quebec
Findings from a study on work-life balance among parents inside and outside Quebec
VIDEO: Sophie Mathieu on Childcare in Quebec

A new video from Reimagining Care/Work describes childcare in Quebec
Mothers’ Experiences with Fly-In, Fly-Out Work (Families, Mobility, and Work)

Summary of a chapter on the impact of “fly-in, fly-out” work on mothers
November 9, 2022
In their chapter “A Juggling Act: Mothering While FIFO,” authors Griffin Kelly, Maria Fernanda Mosquera Garcia, and Dr. Sara Dorow provide a window into the realities and resiliencies of “mothering while FIFO.” They explore the experiences of mothering among women working under FIFO conditions in western Canada (Alberta and British Columbia). As illustrated by the four stories, these conditions create a variety of challenges for becoming and being a mother across different stages of the life course.
This chapter is one of many contributions included in Families, Mobility, and Work, a compilation of articles and other knowledge products based on research from the On the Move Partnership. Published in September 2022 by Memorial University Press, this book is now available in print, as an eBook, and as a free open-access volume available in full on the Memorial University website.
“Managing camp and home ‘selves’ is crucial to keeping one’s sanity as a [fly-in, fly-out] worker; but the demands of motherhood bring clashes and conflicts to these selves, including trying to imagine a future self beyond ‘work’ and ‘mother.’ […] these stresses and adjustments across disparate times and spaces, and across the realities of boom-and-bust cycles, further extend gendered chains of care, quite often to FIFO mothers’ own mothers.” – Griffin Kelly, Maria Fernanda Mosquera Garcia, and Sara Dorow, PhD
Access Families, Mobility, and Work
Chapter abstract
Very little research exists on tradeswomen’s experiences of mobile work, let alone on how mobile work shapes their family lives (Nagy and Teixeira, 2020, is one recent exception). In the context of FIFO (fly-in, fly-out) work, attention to women, family, and motherhood has focused on the spouses of FIFO workers (Kaczmarek and Sibbel, 2008; Swenson and Zvonkovic, 2016) and to some degree on women employed in FIFO professional or camp jobs. Our paper combines findings from two current studies of tradeswomen, predominantly in the oil sands of Alberta, to convey experiences of “mothering while FIFO.” We offer four narrative vignettes that illustrate and humanize the challenges and exclusions faced by FIFO tradeswomen engaged in resource extraction work in western Canada at different stages of mothering: when pregnant on the job, while raising children, and during custody disputes. These stories demonstrate the need for examination of the policies and practices of FIFO-based employers that create barriers to work for mothers.
About the authors
Griffin Kelly is a graduate of the MA thesis program of the Department of Sociology at the University of Alberta, where she completed a thesis on tradeswomen’s experiences of gendered harassment in the oil sands of Alberta.
Maria Fernanda Mosquera Garcia is an MA student in Sociology at the University of Alberta. Her research focuses on Latin Americans’ forced displacement and settlement experiences in Canada. She provides research assistantship for the Mobile Work and Mental Health Project, and has participated in the University of Alberta Prison Project as a research assistant.
Sara Dorow, PhD, MA, BA, is Professor and Chair in the Department of Sociology at the University of Alberta. Her research and teaching are in the areas of mobility, migration, family, work, and gender, using an intersectional, qualitative approach. She was Alberta Team Lead for the On the Move Partnership as part of her long-standing study of the social facets of the oil sands region. Previously she studied issues of family, race, and gender in transnational adoption.
Child Care Policy in Canada: Yesterday, Today, and Tomorrow

Gordon Cleveland reflects on progress in child care policy and next steps.
Research Snapshot: Gender, Affordable Housing, and the “Poverty Gap” in Canada
Highlights from a study on the experiences of women in Calgary who live in affordable housing
Research Snapshot: Access to Postnatal Healthcare and Supports Among Syrian Refugee Mothers

Findings from a study on the postnatal experiences of Syrian refugee mothers in Canada.
Research Snapshot: Impact of Maternal Incarceration on Family Relationships

Findings from a recent study of the effects of incarceration on mothers and their children.
Research Snapshot: Indigenous Doula Care and the Revitalization of Indigenous Knowledge

A summary of a qualitative study on perinatal and childbirth experiences of Indigenous mothers.
Research Snapshot: Family Dynamics and the Canadian Gender Income Gap

A summary of research on families, gender equality, and income in Canada
Research Recap: Gendered Impacts of Supports for Employed Caregivers
Gaby Novoa summarizes new research on the impact of workplace policies on employed caregivers.
Researcher Spotlight: Kim de Laat

Kim de Laat discusses her research on family diversities, inequality and parental leave.
COVID-19 IMPACTS: Newcomer and Refugee Mothers in Canada – Final Report

Final report on COVID-19 IMPACTS: Newcomer and Refugee Mothers in Canada survey.
In Brief: COVID-19 IMPACTS Through a Gender-based Lens

Diana Gerasimov summarizes new findings on the gendered impacts of the pandemic.
REVIEW: Mothers, Mothering, and COVID-19: Dispatches from a Pandemic

Alex Foster-Petrocco reviews a new book exploring the experiences of mothers during COVID-19.
Research Recap: Positive Impacts of Parental Benefits on Couple Relationships
Nathan Battams and Gaby Novoa highlight findings from a study on parental leave and divorce.
Report: COVID-19 and Parenting in Canada

September 3, 2020
In June 2020, the Vanier Institute prepared the report Families “Safe at Home”: The COVID-19 Pandemic and Parenting in Canada for the UN Expert Group Meeting Families in Development: Focus on Modalities for IYF+30, Parenting Education and the Impact of COVID-19. Now available in English and French, this report highlights family experiences, connections and well-being during COVID-19, as well as the current resources, policies, programs and initiatives in place to support families and family life.
Families “Safe at Home” details federal, provincial and territorial resources created to offset, mitigate or alleviate the financial impact that the COVID-19 pandemic has had on families. In addition to government responses, a summary is provided of the diverse range of available services that support families from pre-parenthood to adolescence and that serve parents across Canada, including those who belong to Indigenous, 2SITLGBQ+ and newcomer communities.
The Expert Group Meeting was organized by the Division for Inclusive Social Development (DISD) of the UN Department of Economic and Social affairs (UN DESA), where experts from diverse fields from around the world connected virtually to discuss COVID-19 impacts, assess progress and emerging issues related to parenting and education, and plan for upcoming observances of the 30th anniversary of the International Year of the Family (IYF).
Families “Safe at Home”: The COVID-19 Pandemic and Parenting in Canada
Nora Spinks, Sara MacNaull, Jennifer Kaddatz
Toward the end of 2019, news began to spread around the world about the novel coronavirus (COVID-19). Like many other countries, Canada was facing the possibility of weeks and months with families living in isolation in their homes, changes to school and work schedules, and unknown impacts on family connections and well-being.
In 2020, global citizens around the world are living in and adapting to new ways of life while remaining “safe at home” during the COVID-19 pandemic. Canadians have been striving to respect physical and social distancing guidelines implemented by our governments and based on the recommendations of public health officials since March 10, 2020. For many families, the past three months have included parenting in close quarters with high levels of uncertainty and unpredictability while managing work commitments, fulfilling care responsibilities inside and outside the home, and homeschooling children of all ages. Despite the inability to plan and the unknowns about what the next few weeks and months might look like, most families are maintaining good physical and mental health, taking care of one another and weathering the storm with their neighbours and communities at a distance.
During these unprecedented times, the Vanier Institute of the Family has adjusted its focus to understanding families in Canada in a time of drastic social, economic and environmental change. The daily activities of individuals and families in Canada, what they are thinking, how they are feeling and what they are doing are all important factors to be addressed and understood in the short, medium or long term.
Accordingly, representatives from the Vanier Institute were co-founders of the COVID-19 Social Impacts Network, a multidisciplinary group of some of Canada’s leading experts along with some of their international colleagues. The network has identified important issues, key indicators and relevant socio-demographics to generate evidence-based responses addressing the social and economic dimensions of the COVID-19 crisis in Canada. As well, to understand the experiences of families during the pandemic, the Vanier Institute has internally mobilized knowledge from other available sources, including quantitative data from both government and non-governmental agencies, such as Statistics Canada and UNICEF Canada, as well as qualitative information from individuals, families and organizations across the nation. Analyses of these findings illuminate characteristics of family life both before and during the pandemic, providing insight into what Canadians fear and what they look forward to after public health measures are lifted.
Consistent with its core principles, the Vanier Institute honours and respects the perspectives of diverse families by applying a family lens and Gender-based Analysis Plus (GBA+), whenever possible.1 By examining the impact of the COVID-19 pandemic and any of its associated “costs and consequences,” including fertility patterns, parenting, family relationships, family dynamics and family well-being, the Institute mobilizes knowledge to those who study, serve and support families to make sound evidence-based decisions when designing and implementing policies and programs for all families in Canada.
COVID-19 Pandemic Experience in Canada
As of May 31, 2020, 1.6 million people have been tested for COVID-19 in Canada (approximately 4.5% of the total population). Among them, 5% have tested positive for the virus, with 8% resulting in death.2 Seniors in long-term care facilities who have died of COVID-19 represent approximately 82% of all deaths linked to the virus.3
Families are like all other “systems” during the pandemic – their strengths and weakness are magnified, amplified and intensified as relationships, interactions and behaviours adapt to changes in routine, habits and experiences. Family connections, family well-being and youth experiences have all been dramatically affected.
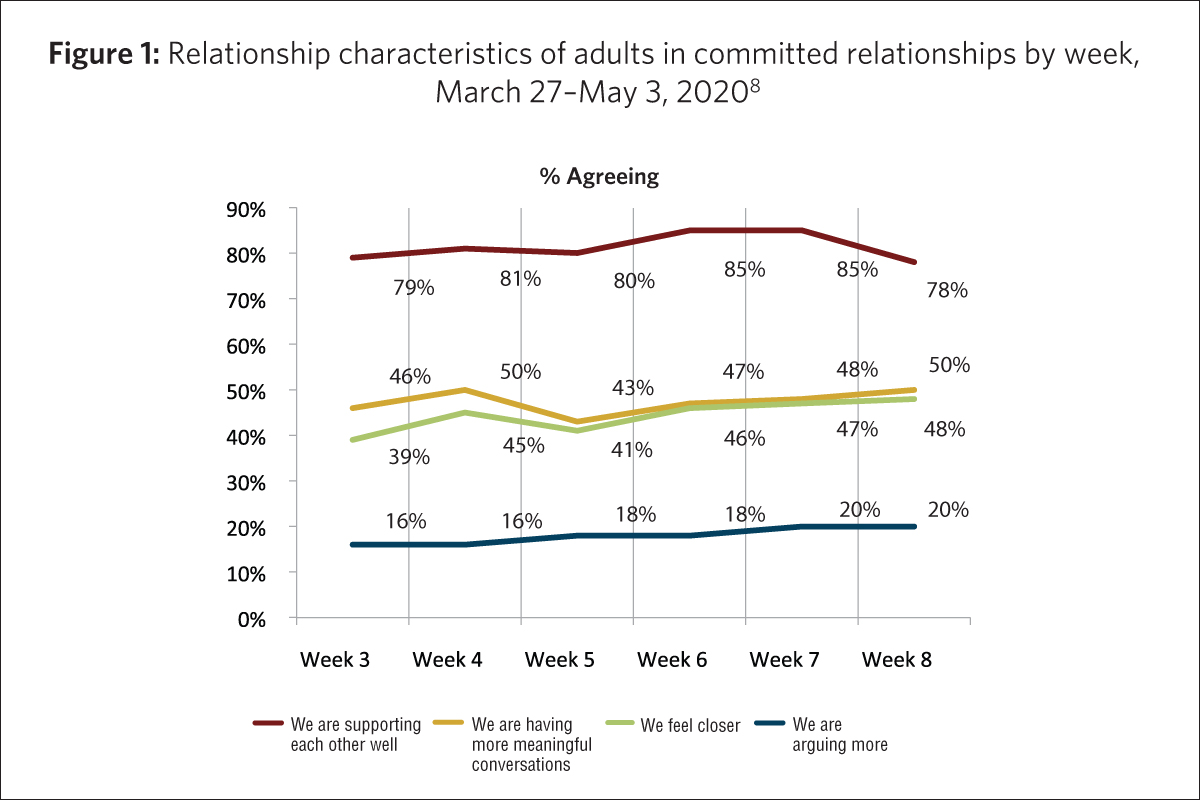
Family Connections
- Approximately 8 in 10 adults (aged 18 and older) who are married or living common-law agreed that they and their spouse were supporting one another well since the start of the COVID-19 pandemic (Fig. 1). This figure varies only slightly for those with children or youth at home (77%) compared with those without children under the age of 18 in the household (82%).4
- Fewer than 2 in 10 adults in committed relationships said they had been arguing more since the start of the pandemic (Fig. 1).5
- Six in 10 parents reported they were talking to their children more often than before the lockdown began.6
- When young kids were in the house, adults were almost twice as likely as those with no children or youth at home to have increased their time spent making art, crafts or music.7
On the other hand…
- One-third of adults said that they were very or extremely concerned about family stress from confinement.9
- 10% of women and 6% of men were very or extremely concerned about the possibility of violence in the home.10, 11
- About 1 in 5 Canadians had senior relatives living in a nursing home or facility, with 92% of females and 78% of men being very or somewhat concerned for their health.12
Family Well-Being
- More than three-quarters of Statistics Canada’s crowdsource participants reported either very good or excellent (46%) or good (31%) mental health during pandemic, in a survey conducted April 24–May 11, 2020.13
- Nearly half (48%) of Statistics Canada’s crowdsource participants said that their mental health was “about the same,” “somewhat better” or “much better” than it had been prior to the start of the pandemic.14
- About half of adults said they felt anxious or nervous or felt sad “very often” or “often” since the beginning of the COVID-19 crisis.15
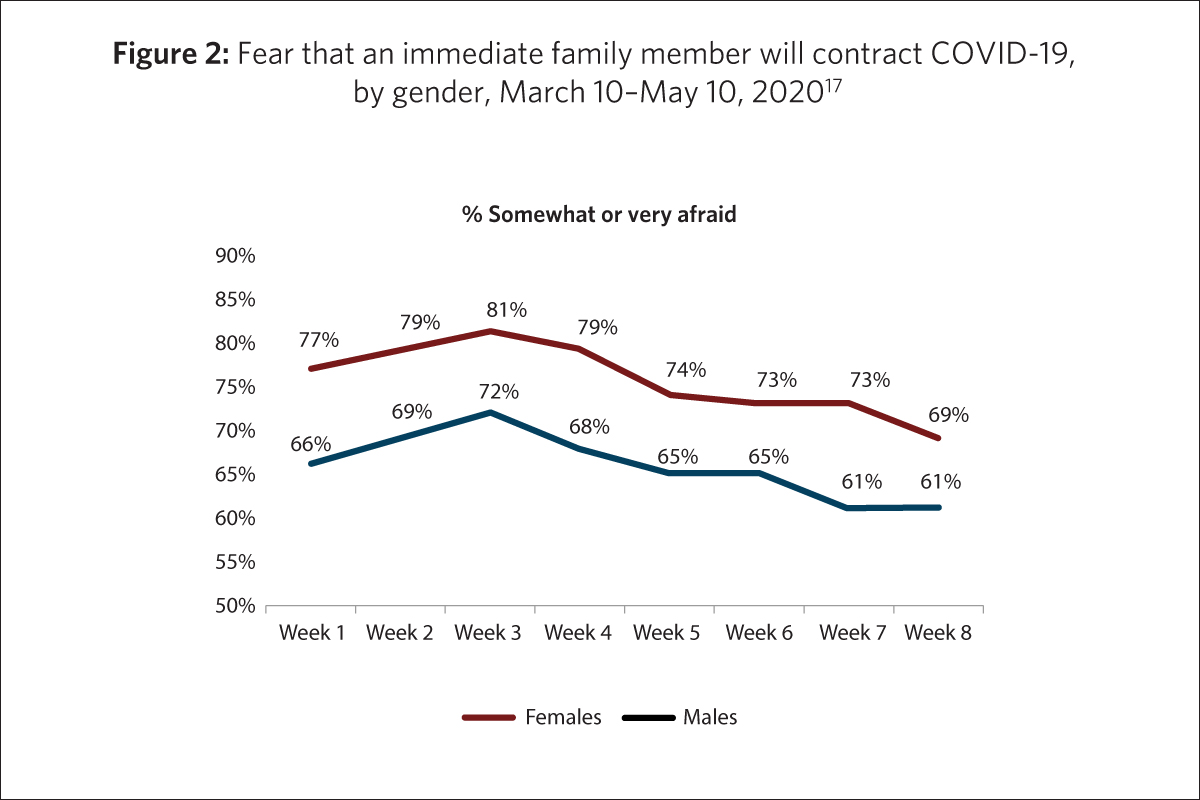
- Regardless of age group or week surveyed, women expressed being more afraid than men that they would contract the virus or that someone in their immediate family would contract it (Fig. 2).16
- Canadians were more afraid of a loved one contracting COVID-19 than they were of contracting it themselves. Adults who were “very” or “extremely”concerned about:
- their own health: 36%
- health of someone in household: 54%
- health of vulnerable people: 79%
- overloading the health care system: 84%18, 19
- More than 4 in 10 of adults living with children under the age of 18 in their home said they “very often” or “often” have had difficulty sleeping since the beginning of the pandemic.20
- When asked to describe how they have been primarily feeling in recent weeks, Canadians were most likely to say they were worried (44%), anxious (41%) and bored (30%); fully one-third (34%) also said they were “grateful.”21
- Women were considerably more likely than men to report experiencing anxiety or nervousness, sadness, irritability or difficulty sleeping during the pandemic.22
- Adults across all age groups continued to exercise during the pandemic, as two-thirds of adults aged 18–34 reported that they were exercising equally as often or more often during the pandemic than they were before it started. The figures were similar for adults aged 35–54 (62%) and aged 55 and older (65%).23
- Younger adults (aged 15–49) were more likely to report an increase in junk food consumption than older adults.24
- Food banks saw a 20% average increase in demand, with some local food banks, such as those in Toronto, Ontario, seeing increases as high as 50%.25
- More than 9 in 10 people aged 15 and older said that the pandemic had not changed their consumption of tobacco nor cannabis.26 Just under 8 in 10 reported that the pandemic had not affected their drinking habits.27
Youth Experiences
- Youth aged 12–19 said they got most of their information about COVID-19 and public health measures from their parents.28
- Older youth, aged 15–17, were more anxious than younger youth, aged 12–14.29
- Among youth aged 15–17, 50% reported that the pandemic had had “a lot” or “some” negative impact on their mental health, compared with 34% of youth aged 12–14. Approximately 4 in 10 youth aged 12–17 reported “a lot” or “some” negative impact on their physical health.30
- Approximately half of children and youth across all age groups missed their friends the most while in isolation.31
- Though 75% of youth claimed to be keeping up with school while in isolation, many were also unmotivated (60%) and disliked the arrangement (57%) (i.e. online learning; virtual classrooms).32
- Many youth said they were doing more housework or chores during the pandemic.33
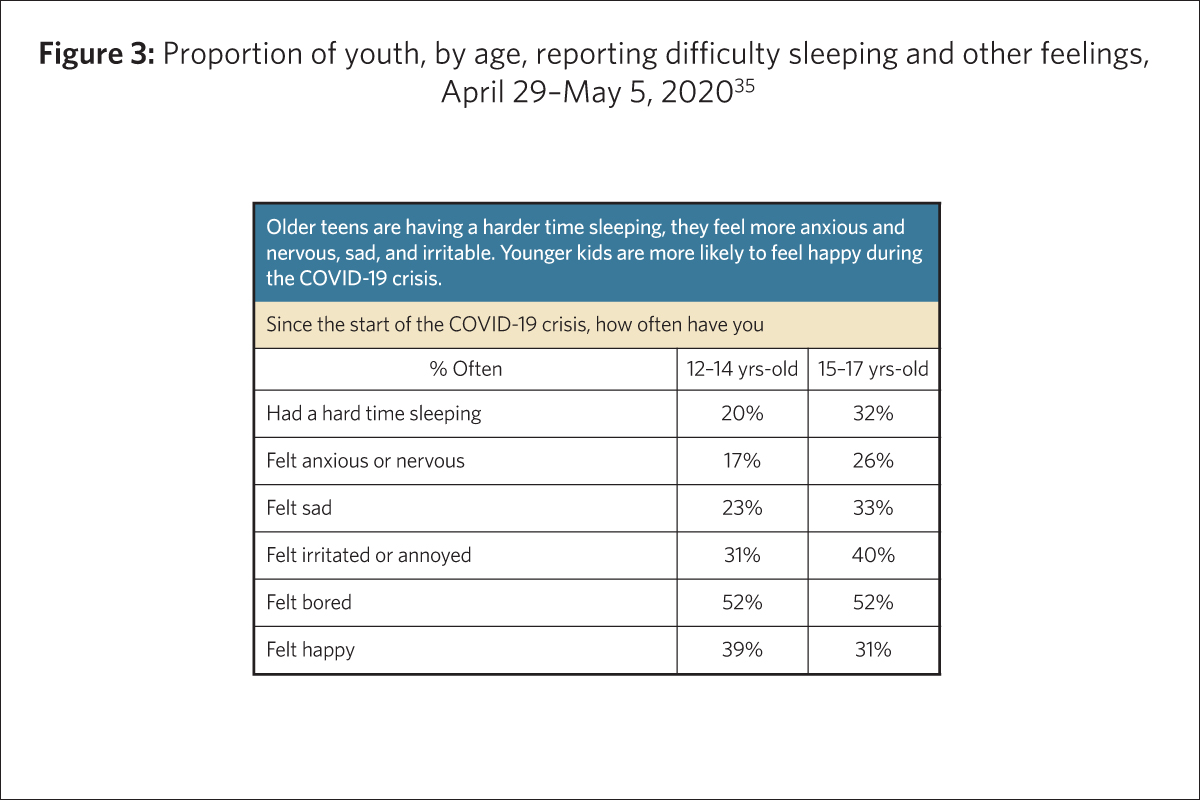
- Older teens (aged 15–17) were having more difficult sleeping, feeling more anxious or nervous, sad and irritable. Younger teens (aged 12–14) were more likely to feel happy than older teens (Fig. 3).34
COVID-19 Pandemic Response in Canada
Since March 2020, the provincial, territorial and federal governments have announced diverse benefits, credits, programs, initiatives and funds to support families across Canada. The purpose of these recent resources is to offset, mitigate or alleviate the financial impact that the COVID-19 pandemic has had on families during this period of uncertainty, including the following:
Temporary Increase to the Canada Child Benefit (CCB)
The Canada Child Benefit (CCB) is a tax-free monthly payment made to eligible families to help with the cost of raising children under the age of 18. The amount of the benefit varies depending on the number of children, the age of the children, marital status and family net income from the previous year’s tax return. The CCB may include the child disability benefit and any related provincial and territorial programs.36
For families already receiving the CCB, an additional $300 per child was added to the benefit in May 2020. For example, a family with two children received $600, in addition to their regular monthly CCB payment, which could be up to a maximum of $553.25 per month per child under the age of 6 and $466.83 per month per child aged 6–17.37, 38
Canada Emergency Response Benefit (CERB)
In April 2020, Canada’s federal government established the Canada Emergency Response Benefit (CERB) to support workers impacted by the COVID-19 pandemic.
The CERB provides $2,000 every four weeks to workers who have lost their income as a result of the pandemic. Eligibility includes adults who have lost their job or who are sick, quarantined or taking care of someone who is sick with COVID-19. It applies to wage earners, contract workers and self-employed individuals who are unable to work. The benefit also allows individuals to earn up to $1,000 per month while collecting CERB.39
As a result of school and child care closures across Canada, the CERB is available to working parents who must stay home without pay to care for their children until schools and child care can safely reopen and welcome back children of all ages.
As of early May 2020, more than 7 million Canadians had applied for CERB since its introduction.40
Mortgage Payment Deferral
Homeowners across Canada who are facing financial hardship due to lack of work or decreased income during the pandemic may be eligible for a mortgage payment deferral of up to six months.
The payment deferral is an agreement between individuals and their mortgage lender, which includes a suspension of all mortgage payment for a specified period of time.41
Special Good and Services Tax Credit
The Goods and Services Tax credit is a tax-free quarterly payment that helps individuals and families with low and modest incomes offset all or part of the Goods and Services Tax (GST) or the Harmonized Sales Tax (HST) that they pay.42
In April 2020, the federal government provided a one-time special payment in April 2020 to those receiving the Goods and Services Tax credit. The average additional benefit was nearly $400 for single individuals and close to $600 for couples.43
Temporary wage top-up for low-income essential workers
The federal government is providing $3 billion to increase the wages of low-income essential workers. Examples of essential workers (though variable by province or territory) may include health care professionals, long-term care facility employees and grocery store employees.
Each province or territory is responsible for determining which workers are eligible for this support and how much they will receive.44
Emergency Relief Support Fund for Parents of Children with Special Needs (Province of British Columbia)
To support parents of children with special needs during the COVID-19 pandemic, the Government of British Columbia created a new Emergency Relief Support Fund. The fund will provide a direct payment of $225 per month to eligible families from April to June 2020 (three months).
The payment may be used to purchase supports that help alleviate stress, such as meal preparation and grocery shopping assistance; homemaking services; caregiver relief support and/or counselling services, online or by phone.45
COVID-19 Income Support Program (Province of Prince Edward Island)
In April 2020, the Government of Prince Edward Island announced financial support for individuals whose income has been impacted as a direct result of the public health state of emergency, as well as additional protocols to keep residents safe.
The COVID-19 Income Support Program will help individuals bridge the gap between their loss of income and Employment Insurance (EI) benefits or the Canada Emergency Response Benefit (CERB) by providing a one-time, taxable payment of $750.46
Support for Families Initiative (Province of Ontario)
In April 2020, the Government of Ontario announced direct financial support to parents while Ontario schools and child care centres remain closed as a result of the COVID-19 pandemic.
The new Support for Families initiative offers a one-time payment of $200 per child aged 0–12 and $250 for those aged 0–21 with special needs.47
Emergency Allowance for Income Assistance Clients (Northwest Territories)
For Income Assistance clients registered in March 2020, the Government of the Northwest Territories provided a one-time emergency allowance to help with a 14-day supply of food and cleaning products as the stores have them available.
The Income Assistance (IA) program is designed for residents who are aged 19 and older and who have a need greater than their income. The emergency allowance received by individuals was $500 and for families it was $1,000.48
Parenting in Canada: Government Priorities, Policies, Programs and Resources
The Government of Canada and the provincial, territorial and Indigenous governments provide support to parents in Canada in myriad ways. In addition to the supports provided to assist families during the COVID-19 pandemic, as described in the previous section, a selection of current priorities, policies, programs and resources that are current and existed pre-pandemic are highlighted below.
Early Learning and Child Care
Early learning and child care needs across Canada are vast and diverse. The Government of Canada is investing in early learning and child care to ensure children get the best start in life. As a first step, the federal, provincial and territorial Ministers responsible for early learning and child care have agreed to a Multilateral Early Learning and Child Care Framework. The new Framework sets the foundation for governments to work toward a shared long-term vision where all children across Canada can experience the enriching environment of quality early learning and child care. The guiding principles of the Framework are to increase quality, accessibility, affordability, flexibility and inclusivity. A distinct Indigenous Early Learning and Child Care Framework was co-developed with Indigenous partners, reflecting the unique cultures and needs of First Nation, Inuit and Métis children across Canada.49, 50
Before- and After-school Care
Canada’s federal government priorities currently include working with the provinces and territories to invest in the creation of up to 250,000 additional before- and after-school spaces for children under the age of 10, at least 10% of which would allow for care during extended hours. Priorities also include decreasing child care fees for before- and after-school programs by 10%.51
Just for You – Parents
“Just for You – Parents” is a federally created web-based list of resources for parents on topics, including alcohol, smoking and drugs; child abuse; childhood diseases and illnesses; educational resources; family issues; healthy living; mental health; parenting tips (childhood development); school health; and work–life balance. Each topic includes a range of subtopics that direct parents through links to the most up-to-date information available in Canada on issues of importance to them and their children.52
Guaranteed Paid Family Leave Program
In 2019, the Minister of Families, Children and Social Development was tasked to work with the Minister of Employment, Workforce Development and Disability Inclusion to improve and integrate the existing Employment Insurance-based system of maternity and parental benefits and work with the province of Quebec on the effective integration with its own parental benefits system.53
- Maternity and Parental Benefits Administered through the Employment Insurance (EI) program in Canada (excluding Quebec), maternity and parental benefits include financial support (i.e. income replacement for eligible workers) to new mothers and parents following the birth or adoption of a child. The number of weeks and amount paid to each parent varies depending on the type of benefit, number of weeks and maximum amount payable (as determined by the government).54 In Quebec, the Quebec Parental Insurance Plan (QPIP) administers the maternity, paternity, parental and adoption benefits. The amount received by parents is also dependent on the type of benefit, number of weeks and maximum amount payable (as determined by the provincial government). In 2019, the average weekly standard parental benefit rate in Canada reached $464.00 per month.55, 56
Modernizing Canada’s Federal Family Laws
On June 21, 2019, Royal Assent was given to amend Canada’s federal family laws related to divorce, parenting and enforcement of family obligations. The first update to family laws in more than 20 years, this initiative will make federal family laws more responsive to the needs of families through changes to the Divorce Act, the Family Orders and Agreements Enforcement Assistance Act, and the Garnishment, Attachment and Pension Diversion Act. The majority of the amendments to the Divorce Act will come into force July 1, 2020, while amendments to the other Acts will take place over two years. The legislation has four key objectives: promote the best interests of the child; address family violence; help to reduce child poverty; and make Canada’s family justice system more accessible and efficient.57
Provincial and Territorial Child Protection Legislation and Policy
The federal, provincial and territorial governments of Canada recognize the importance of surveillance in providing evidence about the contexts, risk factors and types of child maltreatment to inform policy, program, service and awareness interventions. Through their child welfare ministries, the provincial and territorial governments are responsible for assisting children in need of protection; they are also the primary source of administrative data and information related to reported child maltreatment. Preventing and addressing child maltreatment is a complex undertaking that involves the engagement of governments at all levels and in various sectors, including social services, policing, justice and health. At the federal level, the Family Violence Initiative brings together multiple departments to prevent and address family violence, including child maltreatment. The Department of Justice is responsible for the Criminal Code, which includes several forms of child abuse. As the Criminal Code currently stands – which has been debated by advocates and parents alike – section 43 legally allows for the use of corporal punishment on children by select individuals as long as does not exceed what is reasonable under the circumstances.58, 59
Nobody’s Perfect
Introduced nationally in 1987 and currently owned by the Public Health Agency of Canada, Nobody’s Perfect is a facilitated parenting program for parents of children aged 0–5. The program is designed to meet the needs of parents who are young, single, or socially or geographically isolated, or who have low income or limited formal education, and is offered in communities by facilitators to help support parents and young children. It provides parents of young children with a safe place to build on their parenting skills, an opportunity to learn new skills and concepts, and a place to interact with other parents who have children the same age.60
Aboriginal Head Start in Urban and Northern Communities
The Aboriginal Head Start in Urban and Northern Communities (AHSUNC) Program is a national community-based early intervention program funded by the Public Health Agency of Canada. AHSUNC focuses on early childhood development for First Nations, Inuit and Métis children and their families living off-reserve. Since 1995, AHSUNC has provided funding to Indigenous community-based organizations to develop and deliver programs that promote the healthy development of Indigenous preschool children. It supports the spiritual, emotional, intellectual and physical development of Indigenous children, while supporting their parents and guardians as their primary teachers.61
Parenting in Canada: Pre-Parenthood to Adolescence62
For expectant parents (or those considering parenthood), the months leading up to the birth or adoption of a child can be exciting and overwhelming. There are many things to prepare for – including the unexpected – in advance of the little one’s arrival. Support in Canada often includes regular and free visits with an obstetrician-gynecologist, a midwife or other registered health care professionals to ensure healthy growth and development. Programs and services are also available in communities across Canada to prepare and plan for parenthood.
- 2SITLGBQ+ Family Planning Weekend Intensive This two-day program is structured to explore pathways to parenthood and strategies for achieving one’s vision of kinship and family. Participants are encouraged to ask questions, gather information and build community, while exploring topics such as co-parenting, multi-parent and single parent families, pregnancy, kinship struggles and self-advocacy. (LGBTQ+ Parenting Network)
- Preparing for Parenthood Geared toward parents-to-be, this program offers information about how to remain healthy during pregnancy and what to expect during the early days and weeks of parenthood. (EarlyON Child and Family Centres)
- Mommies & Mamas 2B/Daddies & Papas 2B This 12-week course is geared toward gay/lesbian, bisexual and queer men/women who are considering parenthood. The course includes resources and discussions to explore practical, emotional, social, ethical, financial, medical, legal, political and intersectional issues related to becoming a parent. Topics explored include co-parenting, surrogacy, parenting arrangements, non-biological and adoptive parenting, fertility awareness, pre-natal care options and legal issues. (LGBTQ+ Parenting Network)
Newborns and Infants
Caring for a newborn or infant comes with many triumphs and challenges. For parents, programs and services are offered across the country, many free of charge, including visits with pediatricians and registered health care professionals. Postnatal care services vary across regions and communities, which may include informational supports, home visits from a public health nurse or a lay home visitor, or telephone-based support (e.g. Telehealth) from a public health nurse or midwife.63 Organizations across the country also offer drop-in programs for parents, grandparents and caregivers to support healthy child development and attachment.
- Roots of Empathy At the heart of the program are an infant and parent who visit a local classroom every three weeks over the course of the school year. Along with a trained Roots of Empathy Instructor, students observe the baby’s development and feelings. This program provides opportunities for parents and infants to take part in teaching emotional literacy and empathy to children aged 5–12, while strengthening their own bonds to each other. (Roots of Empathy)
- Parenting My Baby Tailored to new parents to provide opportunities to learn, participate in discussions on various topics related to infancy, child development and parenting, as well as opportunities to meet fellow new parents. (EarlyON Child and Family Centres)
- Bellies & Babies This drop-in group is geared toward pregnant women and new parents with babies from birth to one year. The group provides individual and peer support for pregnant women and postnatal mothers and provides resources and support to new parents. Resources include topics such as the importance of early secure attachment, nutrition, breastfeeding, mental health, infant development and parenting. (Sunshine Coast Community Services Society)
- Young Parents Connect This informal support group is geared toward parents and parents-to-be under the age of 26. It provides an opportunity to meet other young parents, ask questions and share concerns. Each session also includes a fun, interactive activity for children and parents together. (EarlyON Child and Family Centres)
Toddlers and Preschoolers
Programs for toddlers and preschoolers include a variety of activities to engage both children and their parents to support healthy child development and parent–child attachment. Programs may include drop-in activities, such as those offered by the Boys and Girls Club of Canada or through municipal recreation centres. The drop-in program – offering dancing, story time, arts and crafts and much more – provides opportunities for parents, caregivers and grandparents to take part in learning activities to create, explore and play. Drop-ins welcome moms, dads, grandparents and caregivers, while also providing opportunities to meet and connect with others within the community.
- Parenting Skills 0–5 This online parenting class is designed for families experiencing challenges, providing parents with a foundational understanding to raise their children during the first five years. Topics in this class include child development and personality, discipline, sleep and nutrition. Parenting skills classes are also available for parents with children aged 5–13 and 13–18. (BC Council for Families)
- Fathering Tailored to fathers, including new dads, those experiencing separation or divorce, teen dads and Indigenous dads, this series of resources provides information on how to navigate the various stages of childhood while providing practical tips in support of both fathers and their children. (BC Council for Families)
- Dad HERO (Helping Everyone Realize Opportunities) This project consists of an 8-week parenting course (offered in select correctional institutions in Canada) and a Dad Group both inside the facility for incarcerated fathers and in the community for fathers who were previously incarcerated. This project was designed to educate and teach fathers about parenting, child development and growth, and their role in their children’s lives. Dad HERO provides parenting education and support connecting fathers with their children and improve their mental health and well-being. (Canadian Families and Corrections Network)
School-Aged Children
As children begin and progress through the formal education system in Canada, they encounter various people (i.e. peers, educators) and influences (i.e. social media). Programs and services for parents of school-aged children provide practical tips, informative resources and opportunities to meet and engage with fellow parents in their communities.
- Parenting School-Age and Adult Children This resource was created to support newcomer parenting programs and address some of the challenges that newcomer parents and caregivers may have with parenting in Canadian society. The goal of the program is to gain effective communication skills, better understand the Canadian school systems and create a safe space for parents and caregivers to address their questions and concerns relating to children integrating into the wider Canadian society and culture. (CMAS)
- Positive Discipline in Everyday Parenting This workshop series promotes non-violent discipline and respects the child as a learner. It is an approach to teaching that helps children succeed, gives them information and supports their growth from infancy to adulthood. (EarlyON Child and Family Centres)
- Newcomer Parent Resource Series Available in 16 languages (e.g. Urdu, Arabic and Russian), this resource series explores various topics of interest tailored to meet the unique needs of immigrant and refugee parents of young children. Topics include Keeping Your Home Language, Guiding Your Child’s Behaviour, Helping Your Child Cope with Stress, Children Learn Through Play, and Listening to and Talking with Your Child. (CMAS)
- Parenting after Separation: Meeting the Challenges This six-week program is geared toward parents who have recently experienced separation from their partner. Parents meet once a week to discuss the challenge associated with parental separation and divorce and learn practical strategies to support their children. (Family Service Toronto)
- Foster Parent Support This program provides direct, outreach-oriented support to foster parents/caregivers and the children/youth in their care. Support workers work directly with the family in their home, in the community or via phone. This program is intended to be flexible in meeting the unique needs of each foster family and can offer a variety of supports, including teaching conflict resolution skills, de-escalation techniques, collaborative problem solving and using strength-based and trauma-informed approaches. (Boys and Girls Club of Canada)
Adolescents
Parenting a teen can be challenge, especially in the rapidly evolving era of technology. Adolescence can also be a difficult time for teens who may be questioning their identity, their purpose and envisioning their goals for the future. Programs for parents of teens recognize the importance of supporting children through adolescence as they transition into adulthood.
- Parents Together This is an ongoing professionally facilitated education and group support program for parents who are experiencing challenges while parenting a teen. This program helps parents address their feelings (e.g. guilty, isolation) and provides opportunities to develop new skills and knowledge that can help decrease conflict in the home between parents and their teen. (Boys and Girls Club of Canada)
- Transceptance This is an ongoing monthly peer support group for parents and caregivers of transgender youth and young adults. The support provides support and education, reduces isolation and stress, and shares information, including strategies for dealing or coping with disclosures. (Central Toronto Youth Services)
- Parenting in the Know This 10-week education and support program to learn more about adolescent development, teen mental health and other common issues that parents experience. Local guest speakers, community resources, practical ideas and connections with others experiencing similar issues help parents feel better equipped to parent their teen. (Boys and Girls Club of Canada)
- Families in TRANSition (FIT) This 10-week program is geared toward parents/caregivers of trans- and gender-questioning youth (aged 13–21) who have recently learned of their child’s gender identity. The program provides support to parents/caregivers to gain tools and knowledge to help improve communication and strengthen their relationship with their youth; learn about social, legal and physical transition options; strengthen skills for managing strong emotions; explore societal/cultural/religious beliefs that impact trans youth and their families; build skills to support their youth and family when facing discrimination, transphobia and/or transmisogyny; and promote youth mental health and resilience. (Central Toronto Youth Services)
Looking Ahead
Families are the most adaptive institution in the world. They are resilient, diverse and strong.
As countries around the world begin to focus on the post-pandemic future, families and family experiences will continue to evolve and adapt. Parents may return to work outside the home, when children return to school and child care, and many will continue to work remotely. Some extracurricular activities will return, while classes like martial arts may continue to be delivered online.
While predicting the future has never been easy, the impact and realities of the global pandemic on families is not yet known, and programs and services may require adjustments in order to support the physical, mental, emotional and social well-being of parents and their children through a trauma-informed lens. Though many families may have been safe at home, some experienced an increase in violence, stress, isolation and anxiety.
Policy and program development, benefits, resources, supports and services will require a comprehensive understanding of families in Canada, their experiences and aspirations; thoughts and fears; and hopes and dreams during this period in time which has evolved and may forecast what lies ahead. The research and innovation behind the many initiatives, including those included in this paper, will help guide evidence-informed decisions; the development, design and implementation of evidence-based programs, policies and practices; and evidence-inspired innovation at all levels of government, community organizations, workplaces and faith communities to ensure families in Canada thrive now and into the future.
Nora Spinks is CEO at the Vanier Institute of the Family.
Sara MacNaull is Program Director at the Vanier Institute ofthe Family.
Jennifer Kaddatz is a senior analyst at the Vanier Institute of the Family.
Published on June 23, 2020
______________________________________________________________________________
This report was originally published on June 23, 2020 on the UN Department of Economic and Social affairs (UN DESA) website as part of the Expert Group Meeting on Families in Development: Focus on Modalities for IYF+30, Parenting Education and the Impact of COVID-19. This event was organized by the Division for Inclusive Social Development (DISD) of UNDESA to convene diverse experts from around the world virtually to discuss the impact of COVID-19 on families, assess progress and emerging issues related to parenting and education, and plan for upcoming observances of the 30th anniversary of the International Year of the Family (IYF).
Appendix A: Organizational and Program Overview
Founded in 1977, the BC Council for Families (BCCF) has been developing and delivering family support resources and training programs to professionals across the province of British Columbia as a way to share knowledge and build community connections. The BCCF offers online classes, resources and programs to support parents and children from infancy to adulthood.
The Boys and Girls Clubs of Canada offer educational, recreational and skills development programs and services to children and youth in communities across Canada. The Clubs strive to provide safe, supportive places where children and youth can experience new opportunities, overcome barriers, build positive relationships and develop confidence and skills for life. Many Clubs also offer programs and services to parents to support child development and attachment.
__________
Founded in 1992, Canadian Families and Corrections Network (CFCN) aims to build stronger and safer communities by assisting families affected by criminal behaviour, incarceration and reintegration. Their work includes developing resources for children, parents and families to understand the correctional system and process in Canada and to support families as they manage the experience of having a loved one incarcerated.
__________
The Central Toronto Youth Services (CTYS) is a community-based, accredited Children’s Mental Health Centre that serves many of Toronto’s most vulnerable youth. Their programs and services meet a diversity of needs and challenges that young people experience, such as serious mental health issues; conflicts with the law; coping with anger, depression, anxiety, marginalization or rejection; and issues of sexual orientation and gender identity.
__________
Founded in 2000, CMAS focuses on caring for immigrant and refugee children by sharing their expertise with immigrant serving organizations and other organizations in the child care field. They currently identify gaps in service and work to create solutions; establish and measure the standards of care; and support services for newcomer families through resources, training and consultations.
__________
EarlyON Child and Family Centres provide opportunities for children from birth to age 6 to participate in play and inquiry-based programs, and support parents and caregivers in their roles. The goal of the EarlyON is to enhance the quality and consistency of child and family programs across Ontario.
__________
For more than 100 years, Family Service Toronto has been supporting individuals and families through counselling, community development, advocacy and public education programs. This includes direct service work of intervention and prevention such as counselling, peer support and education; knowledge building and exchanging activities; and system-level work, including social action, advocacy, community building and working with partners to strengthen the sector.
__________
Founded in 2001 and housed at the Sherbourne Health Centre (in Toronto, Ontario), the LGBTQ+ Parenting Network supports lesbian, gay, bisexual, trans and queer parenting through resource development, training and community organizing. The Network coordinates a wide range of programs and activities with and on behalf of LGBTQ parents, prospective parents and their families, including newsletters, print resources, support groups, social events, research projects, advocacy and training.
__________
For more than 30 years, Roots of Empathy has strived to build caring, peaceful and civil societies through the development of empathy in children and adults. The goals of Roots of Empathy are to foster the development of empathy; develop emotional literacy; reduce levels of bullying, aggression and violence; promote children’s pro-social behaviours; increase knowledge of human development, learning and infant safety; and prepare students for responsible citizenship and responsive parenting.
__________
Since 1974, Sunshine Coast Community Services Society (SCCSS) has provided services for individuals and families along the Sunshine Coast (British Columbia). Programs are focused around child and family counselling; child development and youth services; community action and engagement; domestic violence; and housing.
Notes
- GBA+ is an analytical process used to assess how diverse groups of women, men and non-binary people may experience policies, programs and initiatives. The “plus” in GBA+ acknowledges that GBA goes beyond biological (sex) and socio-cultural (gender) differences. We all have multiple identity factors that intersect to make us who we are; GBA+ also considers many other identity factors, such as race, ethnicity, religion, age, and mental or physical disability. Link: https://cfc-swc.gc.ca/gba-acs/index-en.html
- Government of Canada. “Coronavirus Disease (COVID-19): Outbreak Update” (May 31, 2020). Link: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection.html
- Marc Montgomery, “COVID-19 Deaths: Calls for Government to Take Control of Long Term Care Homes,” Radio-Canada International (May 25, 2020). Link: https://www.rcinet.ca/en/2020/05/25/covid-19-deaths-calls-for-government-to-take-control-of-long-term-care-homes/
- A survey by Leger, the Association for Canadian Studies and the Vanier Institute of the Family, conducted weekly starting in March (beginning March 10–12), through April and May 2020, included approximately 1,500 individuals aged 18 and older, interviewed using computer-assisted web-interviewing technology in a web-based survey. Some weekly surveys included booster samples of specific populations. Using data from the 2016 Census, results were weighted according to gender, age, mother tongue, region, education level and presence of children in the household in order to ensure a representative sample of the population. No margin of error can be associated with a non-probability sample (web panel in this case). However, for comparative purposes, a probability sample of 1,512 respondents would have a margin of error of ±2.52%, 19 times out of 20.
- Ibid.
- Ibid.
- Ibid.
- Ibid.
- Statistics Canada. “Canadian Perspectives Survey Series 1: Impacts of COVID-19,” The Daily (April 8, 2020). Link: https://www150.statcan.gc.ca/n1/daily-quotidien/200408/dq200408c-eng.htm
- Ibid.
- Though data varies, reports have claimed that consultations by the federal government reveal a 20% to 30% increase in violence rates in certain regions which is supported by organizations such as Vancouver’s Battered Women Support Services that has reported a 300% increase in calls related to family violence during the pandemic. Links: https://bit.ly/2OKYsK0, https://bit.ly/2ZOiF8f.
- Survey by Leger, the Association for Canadian Studies and the Vanier Institute of the Family.
- Statistics Canada. “Canadians’ Mental Health During the COVID-19 Pandemic” (May 27, 2020). Link: https://www150.statcan.gc.ca/n1/daily-quotidien/200527/dq200527b-eng.htm
- Ibid.
- Survey by Leger, the Association for Canadian Studies and the Vanier Institute of the Family.
- Ibid.
- Ibid.
- Ibid.
- Canada’s healthcare system is publicly funded, which means that all Canadian residents have reasonable access to medically necessary hospital and physician services without paying out-of-pocket. https://www.canada.ca/en/health-canada/services/canada-health-care-system.html
- Survey by Leger, the Association for Canadian Studies and the Vanier Institute of the Family.
- Angus Reid Institute. “Worry, Gratitude & Boredom: As COVID‑19 Affects Mental, Financial Health, Who Fares Better; Who Is Worse?” (April 27, 2020). Link: http://angusreid.org/covid19-mental-health/
- Survey by Leger, the Association for Canadian Studies and the Vanier Institute of the Family.
- Ibid.
- Statistics Canada, “Canadian Perspectives Survey Series 1: Impacts of COVID-19.”
- Beatrice Britneff, “Food Banks’ Demand Surges Amid COVID-19. Now They Worry About Long-Term Pressures,” Global News (April 15, 2020). Link: https://bit.ly/3boEHRe.
- On October 17, 2018, the use of cannabis for recreation and medicinal purposes among adults became legal in Canada. https://www.justice.gc.ca/eng/cj-jp/cannabis/
- Michelle Rotermann, “Canadians Who Report Lower Self-Perceived Mental Health During the COVID-19 Pandemic More Likely to Report Increased Use of Cannabis, Alcohol and Tobacco,” StatCan COVID-19: Data to Insights for a Better Canada (May 7, 2020). Link: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00008-eng.htm.
- The Association for Canadian Studies’ COVID-19 Social Impacts Network, in partnership with Experiences Canada and the Vanier Institute of the Family, conducted a nation-wide COVID-19 web survey of the 12- to 17-year-old population in Canada from April 29 to May 5. A total of 1191 responses were received, and the probabilistic margin of error was ±3%. Link: https://acs-aec.ca/wp-content/uploads/2020/05/Youth-Survey-Highlights-May-21-2020.pdf
- Ibid.
- Ibid.
- Angus Reid Institute. “Kids & COVID-19: Canadian Children Are Done with School from Home, Fear Falling Behind, and Miss Their Friends” (May 11, 2020). Link: http://angusreid.org/covid19-kids-opening-schools/
- Ibid.
- The Association for Canadian Studies’ COVID-19 Social Impacts Network.
- Ibid.
- Ibid.
- Canada Revenue Agency. “Canada Child Benefit” (April 8, 2020). Link: https://www.canada.ca/en/revenue-agency/services/child-family-benefits/canada-child-benefit-overview.html
- Government of Canada. “Canada’s COVID-19 Economic Response Plan” (May 28, 2020). Link: https://www.canada.ca/en/department-finance/economic-response-plan.html
- Government of Canada. “Canada Child Benefit: How Much You Can Get” (January 27, 2020). Link: https://www.canada.ca
/en/revenue-agency/services/child-family-benefits/canada-child-benefit-overview/canada-child-benefit-we-calculate-your-ccb.html - Government of Canada. “Expanding Access to the Canada Emergency Response Benefit and Proposing a New Wage Boost for Essential Workers” (April 17, 2020). Link: https://www.canada.ca/en/department-finance/news/2020/04/expanding-access-to-the-canada-emergency-response-benefit-and-proposing-a-new-wage-boost-for-essential-workers.html.
- Catherine Cullen and Kristen Everson, “Canadians Who Don’t Qualify for CERB Are Getting It Anyway – And Could Face Consequences,” CBC News (May 2, 2020). Link: https://www.cbc.ca/news/politics/cerb-covid-pandemic-coronavirus-1.5552436
- Government of Canada. “Canada’s COVID-19 Economic Response Plan.”
- Government of Canada. “GST/HST Credit – Overview” (May 28, 2020). Link: https://www.canada.ca/en/revenue-agency/services/child-family-benefits/goods-services-tax-harmonized-sales-tax-gst-hst-credit.html
- Government of Canada. “Canada’s COVID-19 Economic Response Plan.”
- Ibid.
- Province of British Columbia. “Province Provides Emergency Fund for Children with Special Needs” (April 8, 2020). Link: https://news.gov.bc.ca/releases/2020CFD0043-000650
- Government of Prince Edward Island. “Province Announces Additional Income Relief, Stricter Screening Measures for Travelers” (April 1, 2020). Link: https://www.princeedwardisland.ca/en/news/province-announces-additional-income-relief-stricter-screening-measures-travelers
- Government of Ontario. “Ontario Government Supports Families in Response to COVID-19” (April 6, 2020). Link: https://news.ontario.ca/opo/en/2020/04/ontario-government-supports-families-in-response-to-covid-19.html
- Government of Northwest Territories. “Backgrounder and FAQs | Income Security Programs” (n.d.). Link: https://www.gov.nt.ca/sites/flagship/files/documents/back_grounder_faq_income_assistance_measures_en.pdf
- Employment and Social Development Canada. “Early Learning and Child Care” (August 16, 2019). Link: https://www.canada.ca/en/employment-social-development/programs/early-learning-child-care.html
- Government of Canada. “Indigenous Early Learning and Child Care Framework” (September 17, 2018). Link: https://www.canada.ca/en/employment-social-development/programs/indigenous-early-learning/2018-framework.html
- Government of Canada. “Minister of Families, Children and Social Development Mandate Letter” (December 13, 2019). Link: https://pm.gc.ca/en/mandate-letters/2019/12/13/minister-families-children-and-social-development-mandate-letter
- Government of Canada. “Just for You – Parents” (April 20, 2020). Link: https://www.canada.ca/en/health-canada/services/healthy-living/just-for-you/parents.html
- Liberal Party of Canada. “Choose Forward: More Time and Money to Help Families Raise Their Kids.”
- Financial Consumer Agency of Canada. “Maternity and parental leave benefits” (August 17, 2017). Link: https://www.canada.ca/en/financial-consumer-agency/services/starting-family/maternity-parental-leave-benefits.html
- Government of Québec. “Québec Parental Insurance Plan: What Types of Benefits Are Available to Me?” (May 30, 2017).
- Government of Canada. Employment Insurance Monitoring and Assessment Report for the Fiscal Year Beginning April 1, 2017 and Ending March 31, 2018 (June 1, 2019). Link: https://www.canada.ca/en/employment-social-development/programs/ei/ei-list/reports/monitoring2018.html
- Department of Justice. “Strengthening and Modernizing Canada’s Family Justice System” (August 29, 2019). Link: https://www.justice.gc.ca/eng/fl-df/cfl-mdf/01.html
- Government of Canada. Provincial and Territorial Child Protection Legislation and Policy – 2018 (May 13, 2019). Link: https://www.canada.ca/en/public-health/services/publications/health-risks-safety/provincial-territorial-child-protection-legislation-policy-2018.html#2
- Kathy Lynn, “The Canadian Debate on Spanking and Violence Against Children,” The Vanier Institute of the Family (November 15, 2016).
- Nobody’s Perfect. Parent Information (n.d.). Link: http://nobodysperfect.ca/parents/parent-information/
- Public Health Agency of Canada. “Aboriginal Head Start in Urban and Northern Communities (AHSUNC)” (October 23, 2017). Link: https://www.canada.ca/en/public-health/services/health-promotion/childhood-adolescence/programs-initiatives/aboriginal-head-start-urban-northern-communities-ahsunc.html
- Additional information about the organizations mentioned in this section that deliver programs or services to parents can be found in Appendix A.
- The Vanier Institute of the Family. “In Context: Understanding Maternity Care in Canada” (May 11, 2017).
Parents’ Thoughts on Post-Pandemic Future in Canada

Nadine Badets
May 6, 2020
The COVID-19 pandemic restrictions have transformed family life in Canada. With the closure of schools, daycares, restaurants and many businesses, as well as major job losses and new work-from-home measures, many parents and children are spending a lot more time together.
So how do families feel about life after the pandemic? Six weeks of data from the Vanier Institute of the Family, the Association for Canadian Studies and Leger show that families with children are not ready to send them back to school this year, but parents are ready to go back to their workplaces after the pandemic, among other findings from this ongoing series of surveys.1
Fear of coronavirus greater among families caring for children
As of May 6, 2020, children and youth 19 years and younger represent a small portion of COVID-19 cases in Canada (5%).2 Nevertheless, almost 30% of adults living with children and youth under 18 are very afraid that someone in their immediate family will contract COVID-19, compared with 22% of people not living with children3 (fig. 1).

Even so, more than half of adults living with children (56%) said they would support a government policy that relaxes social (physical) distancing restrictions for everyone under 65, whereas 42% of people living without children said they would support this policy.
Most parents don’t want children to attend summer school to catch up
Over 80% of parents are living with their children during the pandemic, and 7% are sharing custody of their children with a parent in a separate household. Six in 10 parents (60%) reported they are now talking to their children more often than before the lockdown. Parents of school-aged children are also navigating the education system with their children as newly instated teachers, tutors and homework helpers. Home schooling is challenging for many families,4 raising concerns about students falling behind.
Most provinces have not yet announced plans to reopen schools, whereas all three territories have confirmed they will keep schools closed until September. However, Quebec has pledged to reopen most elementary schools on May 11 and, as of April 29, 2020, Ontario and Nova Scotia have tentative opening dates closer to June, but their deadlines keep shifting.5 When surveyed, two-thirds (66%) of parents indicate that even if schools in Canada open before the end of June, they would prefer for their children to return to school in September, rather than attend school over the summer (July and/or August) to catch up for missed time.
More than half of parents are ready to return to work but don’t want to use public transit
The COVID-19 pandemic has created enormous job losses across the country,6 and parents living with children who view the COVID-19 outbreak as a “major threat” to their jobs were more likely to report feeling sad and anxious or nervous, compared with people living without children.7
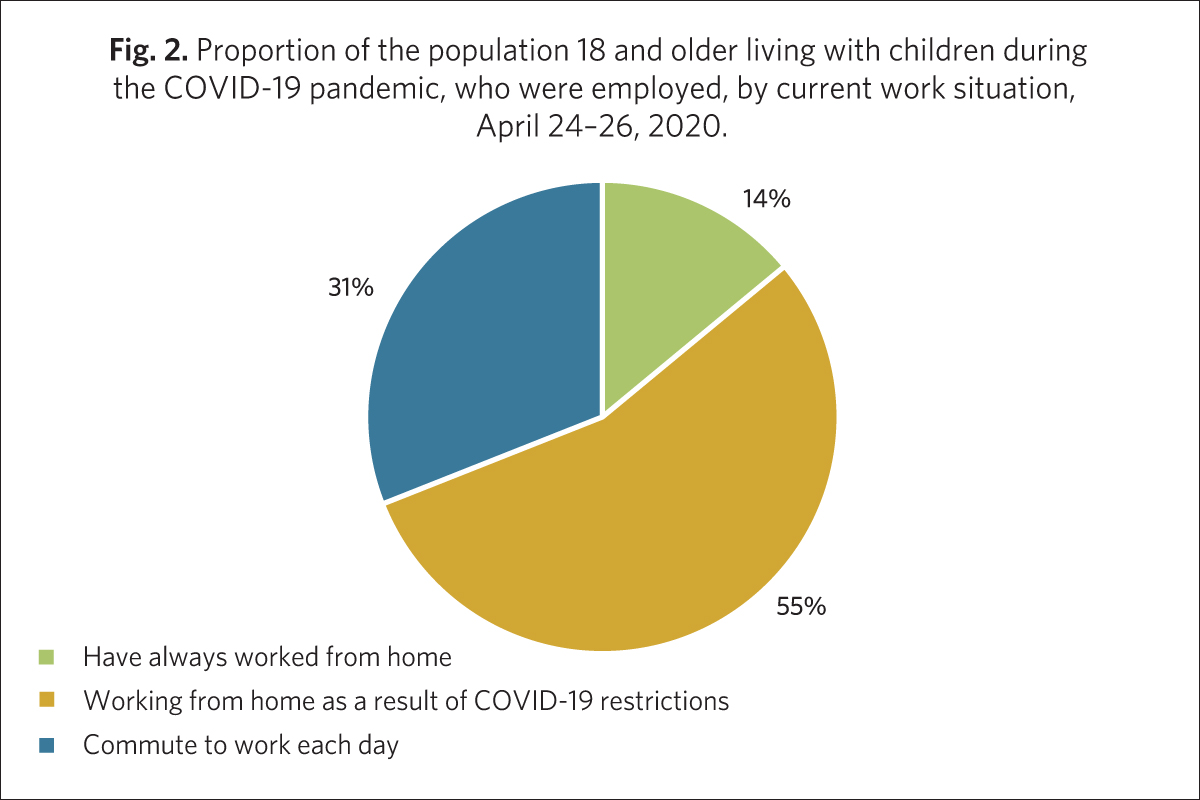
Of those still employed, people living with children were more likely to report satisfaction with the measures their employer put in place to fight COVID-19 (59%) than people without children (37%). This could be because they can work from home and care for their children given that daycares and schools are closed. About 55% of adults living with children reported they are now working from home (fig. 2). People living with children were also more likely to say they would be comfortable returning to their workplace once the COVID-19 restrictions are lifted (54%) than people without children (37%).
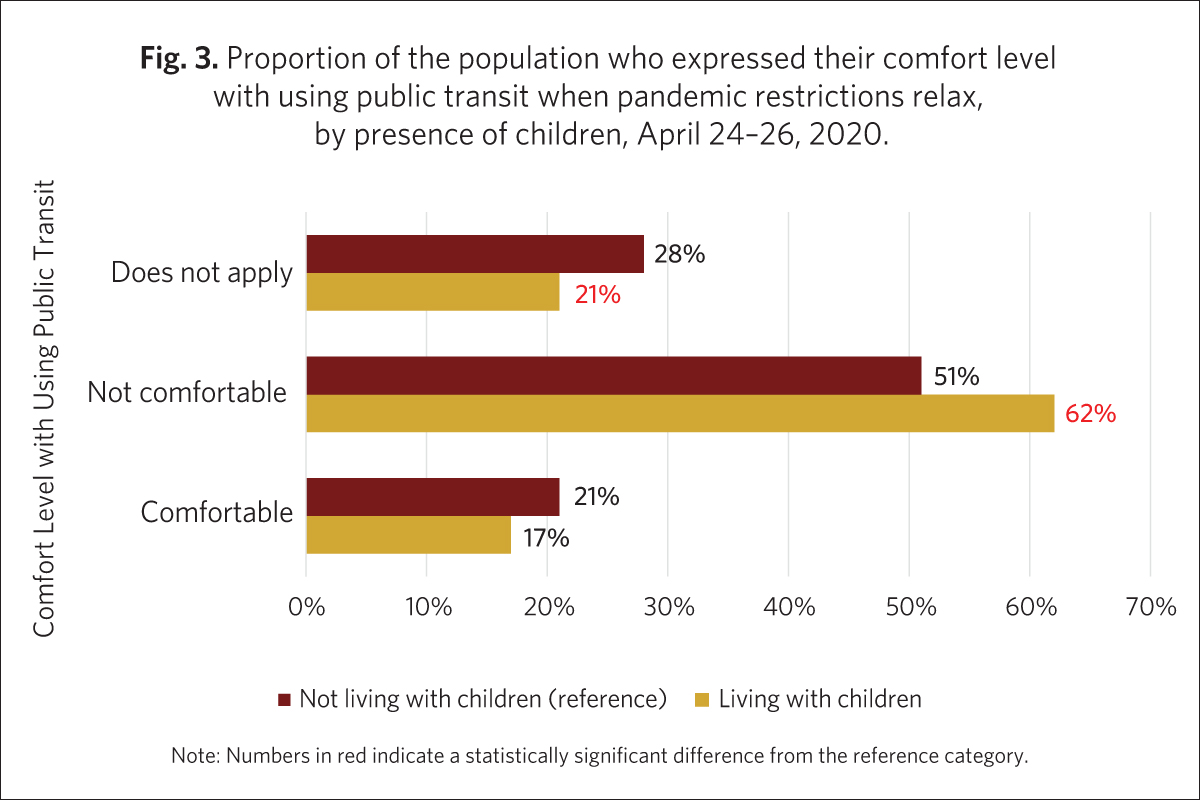
However, more than 60% of parents said they would not be comfortable riding public transit, even when COVID-19 restrictions start being relaxed, which could have implications for commuting once people return to their workplace (fig. 3). Adults living with children were more likely to say they would prefer to commute to work only when needed (39%) than people without children (27%).
Parents abandoning vacation plans, most won’t travel in 2020
In addition to expressing discomfort with commuting in public transit, parents are also not comfortable with travel. About 6 in 10 (59%) adults living with children reported that they had to change vacation plans due to the 2020 coronavirus pandemic, which was likely affected by Canada’s lockdown and borders closing around March break. When asked if they now plan to take a vacation during 2020, 72% of parents said it was unlikely.
Nadine Badets, Vanier Institute on secondment from Statistics Canada
Notes
- A survey by the Vanier Institute of the Family, the Association for Canadian Studies and Leger, conducted March 10–13, March 27–29, April 3–5, April 10–12, April 17–19 and April 24–26, 2020, included approximately 1,500 individuals aged 18 and older, interviewed using computer-assisted web-interviewing technology in a web-based survey. All samples except for the March 10–13 and April 24–26 samples also included booster samples of approximately 500 immigrants. Using data from the 2016 Census, results were weighted according to gender, age, mother tongue, region, education level and presence of children in the household in order to ensure a representative sample of the population. No margin of error can be associated with a non-probability sample (web panel in this case). However, for comparative purposes, a probability sample of 1,512 respondents would have a margin of error of ±2.52%, 19 times out of 20.
- Public Health Agency of Canada, Coronavirus Disease 2019 (COVID-19): Epidemiology Update (accessed May 6, 2020). Link: https://bit.ly/2yXbD68.
- See note 1.
- Jessica Wong, “Frustrated Parents in Ontario Pivot from Official Distance-Learning Program Amid COVID-19,” CBC News (April 30, 2020). Link: https://bit.ly/3aTOMFR.
- CBC Kids News, When Will Your School Reopen? Check Out This Map (April 29, 2020). Link: https://bit.ly/2KMhcGW.
- Statistics Canada, “Labour Force Survey, March 2020,” The Daily (April 9, 2020). Link: https://bit.ly/2YABzPR.
- Jennifer Kaddatz, “Families Struggle to Cope with Financial Impacts of the COVID-19 Pandemic,” Vanier Institute of the Family (April 9, 2020).
Parenting in a Pandemic: A Story and the Stats

Jennifer Kaddatz
April 21, 2020
While trying to ensure that their children are safe, showered and schooled during the COVID-19 pandemic, many parents in Canada, as in other countries, are currently experiencing stress and sleepless nights. According to a survey conducted April 9–12, 2020,1 42% of surveyed adults living with children or youth said that they often/very often had difficulty sleeping since the start of the COVID-19 pandemic. I am one of those parents.
My own family includes three boys (pre-teen and teen), and soon I will be faced with a big credit card bill and some added stress, since the boys left their running shoes in their school lockers on March 12. Having worn boots to school that day, they now having nothing appropriate to wear on a warm Ottawa spring day.
My family has, so far, been extremely lucky in this pandemic. I continue to have a paid job and, like approximately 6.8 million Canadians surveyed by Statistics Canada in the last week of March (39%),2 I’ve been working from home, where it’s easier to avoid germs.
My parents and in-laws are living in isolation on the other side of the country, well cared-for within each of their relationships, like 81% of those in committed couples who say they and their spouse are supporting each other well during the crisis.3 My husband and I also count ourselves within the 79% of couples with kids at home who are supporting each other well during these unusual times.
For my family, the biggest ongoing stressor during the COVID-19 pandemic has, in fact, been related to school – or, more precisely, homeschooling. There are three generations of teachers on my maternal side, but I am not one of them. My boys are attending homeschool on their own for the duration of this pandemic. Elementary and secondary school teachers represent only about 2% of Canada’s labour force,4 which means that the rest of us are not likely qualified for the job.
According to Statistics Canada, 32% of Canadians are very or extremely anxious about family stress resulting from confinement due to the coronavirus.5 I can’t help but wonder what proportion of this anxiety is directly or indirectly related to the effort involved in trying to be a teacher, as well as a parent, while schools are closed.
Some families do not have the resources to enable stress-free homeschooling
Fortunately – or unfortunately, from the perspective of my 14-year-old son – a “pandemic” home education can now be delivered online in most parts of Canada. However, getting this education requires a) a stable, high-speed Internet connection with adequate bandwidth; b) access to a device or, preferably, multiple devices; c) a child who can focus, concentrate and be self-directed; or d) all of the above. The answer here is, of course, d). The question that remains is, therefore, “Is an online education achievable for children in all families across this country?”
A review of available data from official sources provides insight into the family characteristics that may result in greater challenges when it comes to obtaining an online elementary or post-secondary school education during the COVID-19 pandemic and, accordingly, where increased vulnerability might result in a long-term educational gap:
- Low-income households, rural households and Indigenous households are less likely to have the Internet access/speed required to complete online school activities at home. In 2017, only 24% of households in Indigenous communities and 37% of rural households had access to Internet at the minimum speed required to take full advantage of online opportunities, whereas 97% of urban homes had access at that speed or higher.6 In 2018, approximately 4% of households in the lowest income quartile did not have any Internet at home.7
- Low-income families are less likely to have a device other than a mobile device, which could make doing online school work challenging. Nearly one-quarter (24%) of households in the lowest income quartile reported using only mobile devices for accessing the Internet in 2018, three times higher than the share among households in the highest income quartile (8%).8
- Many families have more than one child who is required to complete school work at home, and yet the majority of households may not have enough devices to accomplish this easily. Close to 6 in 10 households (58%) that had Internet access as of 2018 had less than one device per household member.9 This figure was highest (63%) among households in the lowest income quartile.
- Like shoes, assistive devices may not have been sent home before schools were closed, which could impact the ability of children and youth with disabilities to undertake certain educational activities at home. Half of youth with a disability require at least one aid, assistive device or educational accommodation to follow their courses, according to the 2017 Canadian Survey on Disability.10
- Some children do not live in families were the environment is conducive to online learning:
- Almost 19,000 children were victimized by a family member in Canada in 2018 and in 59% of cases, the child was victimized by one of his or her own parents, who most often lived in the same residence.11
- Household food insecurity, which contributes to both poor mental and physical health, is when households cannot afford the quality or quantity of food needed for good health. Not surprisingly, data from 2017–2018 show high rates of food insecurity among households reliant on social assistance (60%) and Employment Insurance or Workers’ Compensation (32%).12
The statistics above only just begin to cover the myriad of intersecting barriers that can impede home learning, not to mention overall well-being, for families in Canada.
For many children and parents, school provides benefits over and above an education – benefits like social and emotional support, nutrition, increased physical exercise and a safe space to be themselves.
I, for one, have seen how many advantages my boys are missing out on since the start of the COVID-19 crisis just by virtue of the fact that they are no longer in school. And, as much as I love having them here at home with me, I cannot wait for them to go back.
Jennifer Kaddatz, Vanier Institute on secondment from Statistics Canada
Notes
- The survey, conducted by the Vanier Institute of the Family, the Association for Canadian Studies and Leger on March 10–13, March 27–29, April 3–5 and April 9–12, 2020, included approximately 1,500 individuals aged 18 and older, interviewed using computer-assisted web-interviewing technology in a web-based survey. The March 27–29, April 3–5 and April 9–12 samples also included booster samples of approximately 500 immigrants. Using data from the 2016 Census, results were weighted according to gender, age, mother tongue, region, education level and presence of children in the household in order to ensure a representative sample of the population. No margin of error can be associated with a non-probability sample (web panel in this case). However, for comparative purposes, a probability sample of 1,512 respondents would have a margin of error of ±2.52%, 19 times out of 20.
- Survey data from Statistics Canada show that during the week of March 22–28, 6.8 million Canadians worked from home (39%), including 4.7 million who don’t usually do so. Link: https://bit.ly/2yqH9t1.
- April 9–12 survey by the Vanier Institute of the Family, the Association for Canadian Studies and Leger (see note 1).
- Statistics Canada, Occupation – National Occupational Classification (NOC) 2016 (693A), Highest Certificate, Diploma or Degree (15), Labour Force Status (3), Age (13A) and Sex (3) for the Labour Force Aged 15 Years and Over in Private Households of Canada, Provinces and Territories, Census Metropolitan Areas and Census Agglomerations, 2016 Census – 25% Sample Data, 2016 Census data tables, Statistics Canada catalogue no. 98-400-X2016295. (November 29, 2017). Link: https://bit.ly/2wSFdsD.
- Statistics Canada, “How Are Canadians Coping with the COVID-19 Situation?,” Infographics, Statistics Canada catalogue no. 11-627-M (April 8, 2020). Link: https://bit.ly/2wVzkuL.
- Minister of Rural Economic Development, High-Speed Access for All: Canada’s Connectivity Strategy, Innovation, Science and Economic Development Canada. Link: https://bit.ly/2XQNecT.
- Statistics Canada, Data to Insights for a Better Canada COVID-19 Pandemic: School Closures and the Online Preparedness of Children, Statistics Canada catalogue no. 45-28-0001 (April 15, 2020). Link: https://bit.ly/2zh73Qh.
- Ibid.
- Ibid.
- Statistics Canada, “Educational Experiences of Youth with Disabilities,” Infographics, Statistics Canada catalogue no. 11-627-M (September 10, 2019). Link: https://bit.ly/2RSInUN.
- Statistics Canada, Family Violence in Canada: A Statistical Profile, 2018, Statistics Canada catalogue no. 85-002-X (December 12, 2019). Link: https://bit.ly/2VlogAG.
- Valerie Tarasuk and Andy Mitchell, Household Food Insecurity in Canada 2017–2018, Toronto: Research to identify policy options to reduce food insecurity (PROOF) (March 2020). Link: https://bit.ly/3cFHDKB.
Facts and Stats: Maternal Mental Health in Canada

Download Facts and Stats: Maternal Mental Health in Canada
Maternal health and well-being is an important public health issue, of which mental health is a key component. Data shows that while most new and expectant mothers report good mental health and high life satisfaction, experiences of postpartum depression (PPD) and anxiety are common in Canada.
Research shows that PPD and poor mental health are detrimental to the well-being of mothers and can, if left untreated, adversely affect infant development (e.g. low birth weight, preterm birth, increased risk of mental health problems in the child later in life), as well as leave partners and other family members (including fathers, who are at an elevated risk for depression or anxiety) feeling overwhelmed.
Fortunately, multiple effective and well-researched treatment options are available to help women recover, and research shows that social and emotional support from partners and other family members throughout the perinatal period can reduce the likelihood of PPD and emotional distress for both mothers and newborns.
This edition of Facts and Stats explores the mental health of new and expectant mothers in Canada, with a focus on family well-being.
Highlights include:
- In 2018–2019, most (60%) mothers who recently gave birth rated their mental health as excellent or very good, while nearly one-quarter (23%) reported feelings consistent with PPD or an anxiety disorder.
- In 2018–2019, 30% of mothers who recently gave birth under the age of 25 reported feelings consistent with PPD or an anxiety disorder, compared with 23% among those 25 or older.
- In 2018–2019, nearly one-third (32%) of recent mothers who reported feelings consistent with PPD or an anxiety disorder said they have received treatment for their emotions or mental health since the birth of their child.
- Maternal mental health is affected by socio-economic status, with research showing higher rates of PPD and depressive symptoms among mothers from marginalized groups, including people living with disabilities; recent migrant mothers, asylum-seekers and refugees; and mothers self-identifying as Black or First Nations.
- Mothers with adverse life experiences are also at a higher risk of developing mental disorders, such as those living in food-insecure households or in emergency or conflict situations, and those who have experienced violence (domestic, sexual or gender-based) or natural disasters.
Download Facts and Stats: Maternal Mental Health in Canada
This resource will continue to be updated as new research and data emerges (previous versions will be continually available on our fact sheets page).
Source information available on the PDF version of this resource.
Report: Symposium on Women and the Workplace
In May 2019, the Vanier Institute of the Family participated in a two-day symposium hosted by Employment and Social Development Canada (ESDC) at the University of Toronto’s Rotman School of Management, where 240 leaders and champions of workplace gender equality and diversity from across Canada shared and discussed leading practices to inspire and advance women’s participation in the workplace.
A report based on these catalytic conversations is now available, and it provides strategies and resources employers can use to advance women’s participation in the workplace with a focus on three key components to advancing workplace gender equality and diversity in Canada:
- Increasing awareness about gender equality and challenging widespread myths
- Changing structures instead of people
- Adopting an intersectional approach to gender equality in the workplace
Women and the workplace – How employers can advance equality and diversity – Report from the Symposium on Women and the Workplace is now available on the ESDC website (also available in PDF format).
Mother’s Day 2019: New Moms Older, More Likely to Be Employed Than in the Past

May 12, 2019 is Mother’s Day, a time to recognize and celebrate the millions of women in Canada who are raising (and co-raising) future generations, often while managing multiple roles at home, in their workplaces and in their communities. The complex relationship between women, work and family across the country has evolved significantly across generations, as new moms are older and more likely to be employed than in the past – trends that are reflected in data recently released from Statistics Canada.
According to recent Vital Statistics data, women across the country are increasingly waiting longer to have children – in fact, the fertility rates of women in their early 20s and late 30s flipped over the past 20 years. Many are instead focusing first on pursuing post-secondary education and career development – continuing a long-term trend observed over the past several decades.
- In 2017, the fertility rate in Canada for women aged 20 to 24 stood at 36 live births per 1,000 women, down from 58 per 1,000 in 2000.1
- In 2017, the fertility rate in Canada for women aged 35 to 39 was 56 live births per 1,000 women, nearly double the rate in 2000 (34 per 1,000).2
- In 2016, the average age of first-time mothers was 29.2 years, up from 27.1 years in 2000.3
Most of these new moms are (and remain) in the paid labour force at the time of birth or adoption of their newborn, often utilizing community supports to facilitate work and family responsibilities.
- In 2016, the employment rate of mothers whose youngest child was aged 0 to 2 was 71%, up from 66% in 2001. As in previous years, this rate was higher in Quebec in 2016 (80%).4
- In 2017, 79% of recent mothers across Canada had insurable employment, 90% of whom received maternity and/or parental benefits.5
- As in previous years, recent moms in Quebec were more likely to have insurable employment (97%) and to have received benefits than their counterparts in the rest of Canada (91%).
- In 2016–17, women accounted for 85% of all parental benefits claims made, down from 89% in 2002.6, 7
Since December 2017, new and expectant parents have been provided with more flexibility regarding the timing and duration of the benefit period.
- New and expectant parents are now able to choose an extended parental benefits option, which allows them to receive their EI parental benefits over a period of up to 18 months at a benefit rate of 33% of average weekly earnings. Compared with the standard parental benefits option, this extends the duration of the benefit period but decreases the benefit rate, which stand at 12 months and 55% of average weekly earnings, respectively.8
- Expectant mothers are also now able to access benefits up to 12 weeks before their due date – four weeks earlier than the previous eight-week limit (no additional weeks are available).9
- In 2017, among recent mothers who had worked as an employee within the previous two years, more than 1 in 5 took or planned to take more than 12 months away from work (21%).10
Published on May 8, 2019
Notes
1 Statistics Canada, Crude Birth Rate, Age-specific Fertility Rates and Total Fertility Rate (Live Births) (Table 13-10-0418-01), page last updated May 2, 2019. Link: https://bit.ly/2PKZV2S.
2 Ibid.
3 Claudine Provencher et al., “Fertility: Overview, 2012 to 2016,” Report on the Demographic Situation in Canada, Statistics Canada catalogue no. 91-209-X (June 5, 2018). Link: https://bit.ly/2JUU872.
4 Martha Friendly et al., “Early Childhood Education and Care in Canada 2016,” Child Care Research and Research Unit (CRRU) (April 2018). Link: https://bit.ly/2TC1BwL.
5 Statistics Canada, “Employment Insurance Coverage Survey, 2017,” The Daily (November 15, 2018). Link: https://bit.ly/2VaYssA.
6 Employment and Social Development Canada, “New Five-Week Employment Insurance Parental Sharing Benefit One Month Away,” News Release (February 18, 2019). Link: https://bit.ly/2TUnXJN.
7 Canada Employment Insurance Commission, Employment Insurance 2002 Monitoring and Assessment Report (March 31, 2003). Link: https://bit.ly/2VRq99k.
8 Learn more in “Webinar Content: Changes to EI Special Benefits,” Transition (January 24, 2018). Link: https://bit.ly/302utBQ.
9 Ibid.
10 Statistics Canada, “Employment Insurance Coverage Survey, 2017.”
Modern Mothers in Canada “Making It Work”

Mother’s Day is just around the corner, a time when Canadians of all ages recognize and honour mothers, grandmothers and, increasingly, great-grandmothers. As women across Canada – including new and expectant mothers – continue to increase their presence in the workforce, families, communities and policy-makers are adapting and reacting to provide flexibility for working moms.
Flexible workplaces helping working moms manage caregiving responsibilities
New and expectant mothers in Canada are increasingly engaged in the workforce, many of whom also provide care to ill and injured family members. Research shows that workplace flexibility is helping moms manage their multiple responsibilities, which in turn can have a positive impact on family well-being.
- In 2016, the labour force participation rate of mothers whose youngest child was under age 6 was 73%, more than double the rate in 1976 (36%).1
- In 2012, 72% of surveyed women said they were satisfied with their work–life balance – the rate was significantly higher for those with a flexible schedule (75%) than for those without a flexible schedule (63%).2
- In 2012, 3 in 10 women were caregivers, 1 in 6 of whom spent 20 or more hours per week providing care.3
- In 2012, 63% of working mothers who were also caregivers said they were satisfied with their work–life balance (compared with 73% among fathers).4
New benefit options providing flexibility to new and expectant working mothers
A number of changes to Canada’s Employment Insurance (EI) maternity and parental benefits5 program went into effect December 3, 2017, providing more flexibility to working mothers (and fathers) through more options regarding the timing and duration of the benefit period.6
- Parents can now choose an extended parental benefits option, which allows them to receive their EI parental benefits over a period of up to 18 months at a benefit rate of 33% of average weekly earnings. This extends the duration of the benefit period but decreases the benefit rate, which stand at 12 months and 55% of average weekly earnings, respectively.7
- Expectant mothers are also now able to file for benefits up to 12 weeks before their due date – four weeks earlier than the previous eight-week limit (no additional weeks are available).
Notes
- Canadian Institute of Child Health, “Module 8, Section 2: Labour Force Participation Rate,” The Health of Canada’s Children and Youth: A CICH Profile (2018). Link: http://bit.ly/2oq4xyZ.
- Statistics Canada, “Satisfaction with Work–Life Balance: Fact Sheet,” Spotlight on Canadians: Results from the General Social Survey, Statistics Canada catalogue no. 89-652-X (page last updated August 12, 2016). Link: http://bit.ly/1S7H2nb.
- Maire Sinha, “Portrait of Caregivers, 2012,” Spotlight on Canadians: Results from the General Social Survey, Statistics Canada catalogue no. 89-652-X (page last updated November 30, 2015). Link: http://bit.ly/1jxgAAm.
- According to Statistics Canada, this is in part because “women are more likely than men to provide care to a family member or friend suffering from a long-term health condition. In addition, those caregivers provide more hours of care on average.” Link: https://bit.ly/1S7H2nb.
- These changes do not apply in Quebec, which has followed the Quebec Parental Insurance Plan (QPIP) since 2006.
- Qualifying standards remain in place: workers require 600 hours of paid employment in the previous year to be eligible, and benefits are generally paid at 55% of average weekly earnings, up to a cap. As of January 1, 2018, the maximum yearly insurable earnings is $51,700 (a maximum amount of $547 per week). Link: https://bit.ly/2IMJv5g.
- The potential overall benefit hasn’t changed: they either can be used up over 12 months or the same amount of money can be stretched out over 18 months. Parents must choose between the standard or extended option when they first apply for EI benefits, and are “locked in” once they do so.
Families in Canada Interactive Timeline

Today’s society and today’s families would have been difficult to imagine, let alone understand, a half-century ago. Data shows that families and family life in Canada have become increasingly diverse and complex across generations – a reality highlighted when one looks at broader trends over time.
But even as families evolve, their impact over the years has remained constant. This is due to the many functions and roles they perform for individuals and communities alike – families are, have been and will continue to be the cornerstone of our society, the engine of our economy and at the centre of our hearts.
Learn about the evolution of families in Canada over the past half-century with our Families in Canada Interactive Timeline – a online resource from the Vanier Institute that highlights trends on diverse topics such as motherhood and fatherhood, family relationships, living arrangements, children and seniors, work–life, health and well-being, family care and much more.
View the Families in Canada Interactive Timeline.*
Full topic list:
- Motherhood
o Maternal age
o Fertility
o Labour force participation
o Education
o Stay-at-home moms
- Fatherhood
o Family relationships
o Employment
o Care and unpaid work
o Work–life
- Demographics
o Life expectancy
o Seniors and elders
o Children and youth
o Immigrant families
- Families and Households
o Family structure
o Family finances
o Household size
o Housing
- Health and Well-Being
o Babies and birth
o Health
o Life expectancy
o Death and dying
View all source information for all statistics in Families in Canada Interactive Timeline.
* Note: The timeline is accessible only via desktop computer and does not work on smartphones.
Published February 8, 2018
In Context: Understanding Maternity Care in Canada

If it takes a village to raise a child, it certainly takes one to bring a child into this world. New and expectant mothers receive care from many people throughout the perinatal period, and the networks and relationships that support them can play a major role in ensuring the health and well-being of new mothers and their newborns.
Childbirth is a milestone, an exciting time when the family grows and a new generation begins. It’s also a period of significant child development – a time of great vulnerability but also of great opportunity to benefit from healthy nurturing.
The experience of pregnancy, childbirth and postnatal care continues to evolve through the generations. Rates of maternal mortality (women dying as a result of pregnancy and childbirth), maternal morbidity (women developing complications as a result of childbirth) and infant mortality all saw significant declines throughout the 20th century following medical advances and improvements in maternal care, nutrition and general living standards.
Maternal and Infant Mortality in Canada
Maternal mortality dropped from 508 deaths per 100,000 live births in 1931 to 7 per 100,000 in 2015.
Infant mortality rates fell from an average of 76 deaths per 1,000 live births in 1931–1935 to 4.9 per 1,000 in 2013.
In the 1800s to the mid-1900s, maternity care in Canada typically took place in the local community and birth occurred in the home, with families and midwives routinely providing care to new and expectant mothers. However, with the development of medicare throughout the 20th century, births and maternity care gradually moved into hospitals and medical clinics, with care being delivered primarily by medical professionals such as doctors and obstetricians – a trend sometimes referred to as the “medicalization of childbirth.”

By the early 1980s, the vast majority of births occurred in regional hospitals, where family physicians or obstetricians were present and assisted by obstetrical nurses. Partners and other family members became largely left out of the childbirth process, often relegated to waiting rooms. Following birth, babies were placed in nurseries, separated from their mothers – a situation that was sometimes traumatic for mothers and their newborns.
Hospitals eventually started allowing the rooming in of mother and baby to facilitate mother–infant attachment and support breastfeeding for the health and well-being of both. During the rooming-in period, nurses would provide new mothers with information for the recovery period, such as instruction about breastfeeding and postnatal care. Throughout this transition in postnatal care practices, the length of time women spent in hospital after having a baby decreased significantly, from an average of nearly five days in 1984–1985 to 1–2 days after vaginal delivery today.


Today, partners are more involved in the birthing process and the perinatal period generally than in the past. Most are present for births, taking on a greater role in these first moments of their children’s lives and in the child rearing in the years that follow. It is more common for couples today to conceptualize childbirth as a shared experience, and many people use language that reflects this trend (“We’re expecting,” etc.).
What is maternity care?
Maternity/perinatal care (hereafter referred to as maternity care) is an umbrella term encompassing a continuum of care provided to the mother and child before, during and after birth. This includes prenatal/antenatal care (care during pregnancy), intranatal care (care during labour and delivery) and postnatal/postpartum care (care for the mother and newborn following birth). Since both mothers and infants undergo major changes throughout the perinatal period, maternity care entails a diverse range of health monitoring and care.
Prenatal/antenatal care (hereafter referred to as prenatal care) monitors and supports the health and well-being of mothers and the developing fetus prior to birth. Fetal health is monitored through screening and diagnostics, such as ultrasounds and blood tests. Health providers also closely track the mother’s health during this period; expectant mothers are provided with information about pregnancy, fetal development, physical comfort, testing, planning for delivery and preparing for parenthood.
Most women (87%) say they were supported by a partner, family or friends throughout the prenatal period.
According to the 2009 Canadian Maternity Experiences Survey, most women (87%) say they were supported by a partner, family or friends throughout the prenatal period. This support, as well as the care provided by health practitioners, can be particularly important during this time when many (57%) women report most days as being stressful. During pregnancy, maternal stress can have an impact on the well-being of the baby, leading to premature birth and/or low birth weight.
Nearly all expectant mothers (95%) report that they started prenatal care in their first trimester. Certain groups were more likely than others to report that they did not start prenatal care in the first trimester, however, such as women aged 15–19 years, those with less than high school education or those who live in low-income households. One of the main reasons cited for not starting care early in the pregnancy was lack of access to a doctor or health care provider.
Intranatal/intrapartum care (hereafter referred to as intranatal care) refers to the care and assistance provided to mothers during labour and childbirth. This involves facilitating the delivery itself in a safe and hygienic manner as well as monitoring the health of mother and child throughout the delivery process. This care is most often provided in hospitals, with mothers receiving care from a variety of health practitioners including obstetricians/gynecologists (reported as the main health care provider during labour and birth by 70% of surveyed mothers), family doctors (15%), nurses or nurse practitioners (5%) or midwives (4%).
Whether provided by a spouse, partner, friend, family member, midwife or doula (or some combination thereof), emotional support during this time is important. Research shows that women who receive continuous social support are more likely to have a shorter labour (i.e. fewer hours) and a vaginal birth, are more likely to report feeling happy with their labour and birth experience and are less likely to use pain medication.
Research shows that women who receive continuous social support are more likely to have a shorter labour and a vaginal birth, and are more likely to report feeling happy with their labour and birth experience.
Postnatal/postpartum care (hereafter referred to as postnatal care) supports mothers and newborns following childbirth, and involves health monitoring and routine assessments to identify any deviation from expected recovery following birth, and to intervene, if necessary.
The postnatal period accounts for the first six weeks of a child’s life – a “critical phase” in which examinations and care from health practitioners play an important role in ensuring the well-being of the mother and child, according to the World Health Organization (WHO).
In their 2013 postnatal care guidelines, WHO outlines best practices including postnatal care in the first 24 hours to all mothers and babies (regardless of where the birth occurs), ensuring that healthy women and their newborns stay at a health facility at least 24 hours and are not discharged early, and have at least four postnatal checkups in the first 6 weeks following childbirth.
According to the Maternity Experiences Survey, more than 7 in 10 women (73%) rated their health as “excellent” or “very good” by 5 to 14 months postpartum. However, more than 4 in 10 women in Canada (43%) said they experienced a “great deal” of problems with at least one postpartum health issue during the first three months following childbirth, such as breast pain (16% of women), pain in the vaginal area or in the area of the caesarean incision (15%) and back pain (12%).
Postnatal support can be important in mitigating postpartum depression, which is reported by 10%–15% of mothers in developed countries. Research has shown that maternal stress during pregnancy, the availability of social support and a prior diagnosis of depression are all significantly associated with developing postpartum depression. Studies have also shown that emotional support from partners and other family members throughout the perinatal period can reduce the likelihood for postpartum depression and emotional distress for mothers and newborns.
Postnatal care services vary across regions and communities in Canada. These can include informational supports, home visits from a public health nurse or a lay home visitor, or telephone-based support from a public health nurse or midwife.
Privately delivered postnatal services have become more prevalent over the past several decades, with postpartum doulas advertising high-intensity supports such as newborn care, breast- and bottle-feeding support, child-minding services, meal preparation, household chores and more. However, these private services often involve out-of-pocket costs that can limit accessibility for some families.

Who provides maternity care?
In addition to the care and support provided by family members and friends, modern maternity care is delivered by a range of health practitioners including family physicians, obstetricians/gynecologists, nurses, nurse practitioners, midwives and birth doulas – all of whom make unique contributions in the continuum of care.
Family physicians provide care to most new mothers throughout the perinatal period and can be involved in all stages of maternity and infant care, though not all provide the full range of care. Fewer physicians across Canada are providing maternity care than in previous decades: the share of family physicians in Canada delivering babies declined from 20% in 1997 to 10.5% in 2010. Today, a growing number of care tasks and responsibilities are being delivered by other medical practitioners, such as obstetricians and midwives.
Most family physicians who report being involved in maternity and newborn care provide “shared care,” offering prenatal care to a certain point (often between 24 and 32 weeks), after which they transfer care to another provider (e.g. obstetricians, midwives or another family physician who delivers babies). Some attend deliveries, but rates vary widely between provinces and the availability of other health providers.
Obstetricians and gynecologists (OB/GYNs) are providing a growing amount of intranatal care in Canada – though not all do so, and rates vary across the provinces. With specialized knowledge and expertise in pregnancy, childbirth and female sexual and reproductive health care (including surgical training, such as caesarian sections), many also serve as consultants to other physicians and are involved in high-risk pregnancies.
Nurses constitute the largest group of maternity care providers in Canada. They can be involved throughout the entire perinatal period, providing a range of care services including childbirth education, pre-birth home care services to women in high-risk situations, assistance during childbirth and sometimes follow-up care to new mothers. Following childbirth, nurses often provide information to new mothers while preparing them for discharge, educating them about topics such as breastfeeding, bathing, jaundice, safe sleep, postpartum mental health, nutrition and more.
Nurse practitioners (NPs) are registered nurses who play a wide variety of roles in health care. They sometimes serve as primary care providers for low-risk pregnancies, performing a variety of tasks such as physical examinations, screening and diagnostic tests, and postnatal care. When providing or facilitating maternity care, NPs often work in interdisciplinary teams with other health professionals such as physicians and midwives. In hospital settings, they also work in labour and delivery units, postpartum units, neonatal intensive care units and outpatient clinics. Due to the breadth of their training and expertise, NPs play important roles in rural and remote communities, where many provide a full range of health care services.
Due to the breadth of their training and expertise, nurse practitioners play important roles in rural and remote communities, where many provide a full range of health care services.
Midwives provide primary care to expectant and new mothers throughout the entire perinatal period, and are playing a growing role in modern maternity care in Canada. They provide a range of care services, including ordering and receiving tests, accompanying women at home or in birthing centres, admitting women for hospital births, as well as assisting with breastfeeding, the early days of parenting and monitoring postpartum healing. Midwives work collaboratively, consulting with, or referring to, other medical professionals when appropriate.
The role of midwives has evolved over the past several decades, with a growing number assisting in all settings where care may be needed – at home, in the community and in hospitals, clinics or health units. There has been increasing emphasis on specialization and training, as midwives have become recognized by and incorporated into most (but not all) provincial/territorial health care systems across the country.

Doulas provide non-clinical/medical support, working with new mothers and their families as well as health care practitioners such as physicians, midwives and nurses. Doulas are not regulated; they focus largely on emotional and informational support, and they do not provide direct health care or deliver babies.
There are different types of doulas for different stages in the childbirth process. Antepartum doulas provide emotional, physical and informational support during the prenatal period. This can include informing new mothers and their families about support groups, techniques for enhancing physical comfort and helping with home care tasks such as errands and meal preparation. Birth doulas support new mothers and their partners during labour and delivery, including emotional and informational assistance and supporting physical comfort. Postpartum doulas support new mothers after the baby is born, providing information about topics such as infant feeding and soothing techniques, and sometimes helping with light housework and childcare.
Perinatologists provide care in the event of high-risk pregnancies (e.g. pregnancy in the context of chronic maternal health conditions, multiple births or genetic diagnoses). They are trained as OB/GYNs and then receive specialized education to facilitate complicated pregnancies. OB/GYNs refer patients to perinatologists when needed, but continue to work collaboratively to support maternal health.
Unique experiences: childbirth in rural and remote areas in Canada
Maternity care in rural and remote areas (including Canada’s northern regions) faces unique challenges due to distances from medical facilities and specialized equipment, less peer support for care providers, as well as a limited number of physicians available for on-call services, and fewer caesarean section and anaesthesia capabilities/services compared with urban centres.
Rural maternity care is most often provided by teams of family physicians, nurses and midwives – in fact, in some communities, they’re the only health practitioners providing maternity care. Rural family physicians are far more likely to provide obstetrical care than their urban counterparts, though over the past several decades, many rural communities have seen a reduction in the number of family physicians providing maternity care and closures of maternity wards.
Due to the limited availability of maternity care providers and services in rural and remote regions, many expectant mothers travel to urban centres to give birth. According to a 2013 report from the Canadian Institute for Health Information, more than two-thirds of rural women in Canada (67%) report that they gave birth in urban hospitals, 17% of whom travelled more than two hours to deliver their babies. Rates are far higher in the North: two-thirds of surveyed mothers in Nunavut and half of those in the Northwest Territories report that they gave birth away from their home community.
Two-thirds of surveyed mothers in Nunavut and half of those in the Northwest Territories report that they gave birth away from their home community.
This has an impact on the well-being of many Indigenous women living in northern regions, many of whom have had to fly to hospitals far from their homes, land, languages and communities to receive maternity care at tertiary or secondary care hospitals (see Indigenous Midwifery in Canada textbox). When surveyed, the majority of mothers reported that leaving home to have their babies was a stressful experience and that it had a negative impact on their families. In April 2016, the federal government announced that it would provide financial compensation to allow someone to travel with Indigenous women who need to leave their communities to give birth.
The number of community hospitals offering obstetrical care in northern regions has fallen since the 1980s. However, a number of birthing centres have opened to fill this care gap, such as in Puvirnituq (Nunavik), Rankin Inlet (Nunavut) and in Inukjuak (Quebec). These facilities have helped women with low-risk pregnancies remain in their communities; however, those with complications or requiring a caesarian birth often still have to travel to give birth.

Unique experiences: new and expectant mothers new to Canada
Canada is home to many immigrant families, which have represented a growing share of the total population. In 1961, 16% of people in Canada reported that they were born outside the country – a rate that increased to 21% by 2011.
Immigration has an impact on the maternity experiences, such as when women decide to have children. Research shows that immigrants have relatively fewer births in the two-year period before migration, which is often followed by a “rebound” in fertility afterward. According to researchers Goldstein and Goldstein, “Fertility preferences of movers may more closely resemble those of the destination country than those of the source country even before they arrive.”
Studies have explored a number of reasons why fertility can be affected by the immigration experience, including temporary separation of spouses during the migration process, a conscious decision to delay childbearing until access to supports such as child allowances is ensured and economic disruption during migration and in the early period (while parents are securing paid employment).
Recent immigrants are significantly more likely than their Canadian-born counterparts to live in multi-generational households (those with three or more generations living under one roof); 21% of immigrants aged 45 and older who arrived in Canada between 2006 and 2011 reported that they live in shared homes, compared with 3% of the Canadian-born population. As such, new and expectant mothers in multi-generational homes may benefit from having more family members nearby to provide care and support.
With regard to accessing maternity care services, research has shown that many immigrant women generally have the opportunity to receive the necessary maternity care services, but rates of satisfaction with maternity care vary greatly across Canada. Some report having faced barriers to accessing and utilizing maternity care services, including (but not limited to) a lack of information about or awareness of the services (sometimes the result of language barriers), insufficient support to access the services (i.e. navigation of the health care system) and discordant expectations between immigrant women and service providers. In some areas, doulas provide valuable emotional, informational and navigation support to immigrant women during the perinatal period.
Social support (e.g. from family, friends and community members) has been identified by immigrant parents as a key factor in accessing maternity care. This circle of support can play an important role in connecting new and expectant mothers from outside Canada with maternity care, and can work with health care and service providers to ensure these women receive “culturally congruent and culturally safe” maternity care.

Maternity care: supporting Canada’s growing families
Pregnancy and childbirth are major life events, not only for new mothers, but also for their families, friends and communities. While there have been many changes in family experiences over the generations regarding pregnancy, childbirth and the postnatal period, there have also been some constant threads: the value and importance of quality care, the diversity of experiences across Canada, and the joy and excitement that can accompany this memorable and life-changing milestone.
Download this article in PDF format.
This content was reviewed by Dr. Marilyn Trenholme Counsell, OC, MA, MD, retired family physician and former Lieutenant Governor (New Brunswick), former Minister of Family (N.B.) and Senator (N.B.).
All references and source information can be found in the PDF version of this article.
Published May 11, 2017
A Snapshot of Women, Work and Family in Canada
Canada is home to more than 18 million women (9.8 million of whom are mothers), many of whom fulfill multiple responsibilities at home, at work and in the community. Over many generations, women in Canada have had diverse employment experiences that continue to evolve and change. These experiences have differed significantly from those of men, and there is a great deal of diversity in the experiences among women, which are impacted by a variety of factors including (but not limited to) cultural norms and expectations, family status, disability and a variety of demographic characteristics.
To explore the diverse and evolving work and family experiences of women in Canada, the Vanier Institute of the Family has created A Snapshot of Women, Work and Family in Canada. This publication is a companion piece to our Fifty Years of Women, Work and Family in Canada timeline, providing visually engaging data about the diverse work and family experiences of women across Canada.
Highlights include:
- The share of all core working-aged women (25 to 54 years) who are in the labour force has increased significantly across generations, from 35% in 1964 to 82% in 2016.
- Employment rates vary among different groups of core working-aged women, including those who are recently immigrated (53%), women reporting an Aboriginal identity (67%) and those living with a disability (52% to 56%, depending on the age subgroup).
- On average, women without children earn 12% more per hour than those with children – a wage gap sometimes referred to as the “mommy tax.”
- Nearly one-third (32%) of women aged 25 to 44 who were employed part-time in 2016 said that they were working part-time because they were caring for children.
- 70% of mothers with children aged 5 and under were employed in 2015, compared with only 32% in 1976.
- In 2013, 11% of all recent mothers inside Quebec and 36% in the rest of Canada, respectively, did not receive maternity and/or parental leave benefits – a difference attributed to the various EI eligibility regimes in the provinces.
- 72% of all surveyed mothers in Canada report being satisfied with their work–life balance, but this rate falls to 63% for those who are also caregivers.
- 75% of working mothers with a flexible work schedule report being satisfied with their work–life balance – a rate that falls to 69% for those without flexibility.
This bilingual resource will be updated periodically as new data emerges. Sign up for our monthly e-newsletter to find out about updates, as well as other news about publications, projects and initiatives from the Vanier Institute.
Download A Snapshot of Women, Work and Family in Canada from the Vanier Institute of the Family.
Published on May 9, 2017
Infographic: Women, Caregiving and Work in Canada
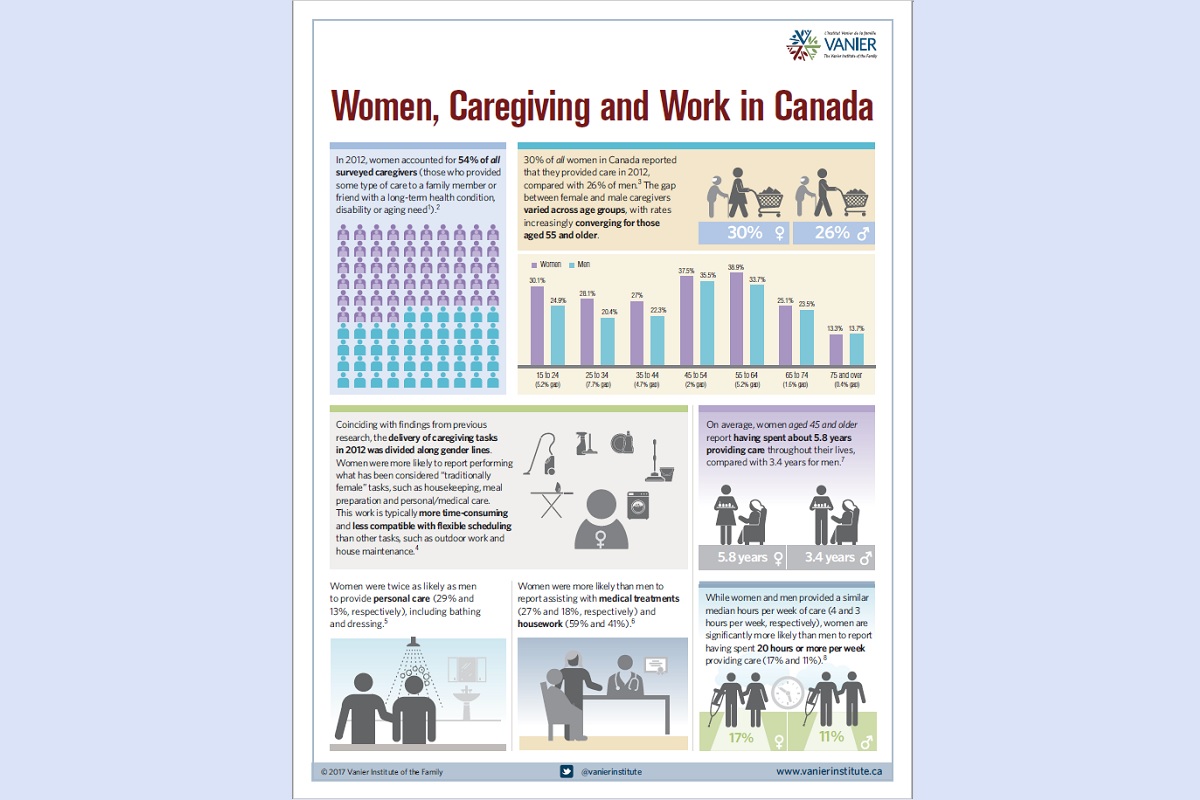
Caregiving is a fact of life and a common family experience in Canada. At some point in their lives, most family members have provided – or will provide – care to a family member or friend with a long-term health condition, disability or aging need. However, Canadians don’t share a single narrative or caregiving experience, as social, economic, cultural and environmental factors shape who is expected to provide care, what kind of care they provide and the consequences of managing caregiving in addition to paid work.
And while the gap between women and men has lessened over the past generation, caregivers have historically been disproportionately women, and this remains true today. Research also shows that on average, women in Canada devote more time to caregiving tasks than men and are more likely to experience negative consequences as a result of their caregiving.
Our new infographic Women, Caregiving and Work in Canada explores family caregiving and work in Canada with a focus on women.
Highlights include:
- 30% of all women in Canada reported that they provided care in 2012.
- Women aged 45 and older reported having spent an estimated 5.8 years providing care throughout their lives, compared with 3.4 years for men.
- Women are significantly more likely than men to report having spent 20 hours or more per week providing care (17% and 11%, respectively).
- An estimated 72% of women caregivers aged 45 to 65 in Canada are also employed.
- Women reported experiencing a variety of employment impacts as a result of their caregiving responsibilities: 30% reported missing at least one full day of work; 6.4% retired early, quit or lost their paid job; and 4.7% turned down a job offer or promotion.
- Estimates show that women caregivers in Canada lost an aggregated $221 million in wages annually between 2003 and 2008 due to absenteeism, reducing work hours or leaving employment entirely.
- Among women caregivers who have access to flexible work arrangements, half (47%) feel they cannot utilize these options without it having a negative impact on their careers.
Download the Women, Caregiving and Work in Canada infographic from the Vanier Institute of the Family.
Supporting the Health of Mothers and Their Babies in the Context of Incarceration

Dr. Ruth Elwood Martin and Brenda Tole
When a friend told Ruth Elwood Martin that there was a need for a part-time family physician to work in a women’s correctional centre, her immediate thought was that there was no way she could work in a prison clinic. She perceived that it was the lowest kind of medical job, only for those doctors who were unable to find any other type of work.
Ruth is not sure what drew her to start practising medicine in a prison, but she did. On that first day in 1994, she felt like she was visiting another planet, passing through those gates, experiencing another world and learning from the people inside it. Ruth saw more pathology and more tragic medical diagnoses than she had seen in a year in her regular family practice in Vancouver’s West Side.
In the clinic, women told her about traumatic events they endured as children, young teenagers and women. Ruth would put down her pen, bearing witness to their lives, and listen to medical and social histories she could not imagine enduring. That first day in her new position changed Ruth’s life forever and she knew that prison health would become her calling. Ruth has often reflected that if she had been dealt the same childhood cards as the women she met, she might be sitting in their chairs.
In 2003, Brenda Tole was assigned to oversee the remodelling of an older facility that had housed provincially incarcerated men and to open it as the “Alouette Correctional Centre for Women” (ACCW), a medium-security facility to house provincially sentenced women. If you are a parent with school-aged children, you will have noticed how the school principal greatly influences the overall ethos of a school. In a similar manner, the warden of a prison influences the ethos of the institution, which in turn influences the overall health of the inmates.
From the day it opened in 2004, Brenda shaped the tone and ethos of ACCW. She maintained that if you expect both staff and incarcerated individuals to treat each other with respect, they will rise to meet those expectations, at least most of the time. That’s how she planned and that’s how she ran ACCW, not on the basis that 1% of the population may breach those expectations.
Brenda knew that the more she gave people opportunities, the more they valued the opportunities and responded positively. The more she gave responsibility to the women for doing things themselves, and the more she talked with the staff about her plans, the better the situation would be for everyone.
During a meeting of key health care players planning for health care delivery at the new ACCW, Brenda met Sarah Payne, the director of Fir Square at BC Women’s Hospital, a maternity unit for substance-using mothers. Babies who remained with moms at Fir Square had positive health outcomes compared with the health of babies that were taken away from their moms at birth.1 Sarah asked Brenda to consider the possibility that babies born to incarcerated mothers who came to the BC Women’s Hospital for their delivery might return with their mothers to ACCW, in order to foster breastfeeding, attachment and nurturing.
Separation through incarceration negatively affects the health of new mothers and their infants
With peer-reviewed academic literature growing on the subject, Brenda had good reason to consider this proposal. Evidence shows that one of the most compelling motivators for incarcerated women is pregnancy and their children. International correctional practices that promote contact between women and their children have shown benefits for both. Positive results have been seen in visits, email, tapes, telephone calls and letters. Children of incarcerated women are negatively impacted if the contact with their mother is limited or absent. Although it is accepted around the world that nursing infants and/or small children benefit from remaining with their incarcerated mothers, this was rarely seen in Canada at that time.
Many incarcerated women have dependent children. Worldwide, an estimated 6% of incarcerated women are pregnant while serving prison time.2 An estimated 20,000 children each year are affected by the incarceration of their mothers in Canada,3 where women tend to be held in correctional centres that are large distances from their children and families due to the limited number of correctional facilities for women across the country.
The provision of mother–child units to women in prison who have given birth to their infants while incarcerated is considered normal practice in most countries in the world. Published reports of such units exist for 22 countries, including England, Wales, Australia, Brazil, Denmark, Finland, Germany, Greece, Italy, the Netherlands, New Zealand, Russia, Spain, Sweden, Switzerland, some US states, Kyrgyzstan, Ghana, Egypt, Mexico, India and Chile.4, 5, 6
One of the reasons for keeping incarcerated mothers with their newborn babies is that it facilitates breastfeeding, which the World Health Organization reports has health benefits for the infant and new mother.7 According to international health experts, babies should be exclusively breastfed until they are six months old if possible, and then continue to be breastfed on demand until they are two years of age. Babies who are not breastfed may be at increased risk for diabetes, allergies and gastrointestinal and respiratory infections.8
In addition to the well-known health and nutritional benefits, some research has shown that breastfeeding can contribute to psychosocial development9 – the associated physical contact, eye contact and the quality of feeding promote mother–child attachment. However, establishing and maintaining breastfeeding on demand is not possible unless mothers and babies can be housed together with 24-hour contact.
Typically, mothers who return to prison without their babies after giving birth are prescribed milk-binding pills and are often prescribed antidepressants. In this situation, many mothers experience profound grief and debilitating guilt, despair and hopelessness. Many resort to substance use as a coping strategy.
Mother–child unit developed to support well-being of incarcerated mothers and their babies
In 2005, Brenda asked Ruth, “As the prison physician, what is your opinion about the idea of incarcerated women who deliver babies in hospital being able to return here with their babies?” Ruth felt it was the most sensible idea she had heard in years, and she then expanded her prison medical practice to perform new roles, such as newborn examinations, breastfeeding coaching and addressing medical questions about newborns.
Through collaboration and partnership with several other ministries and community agencies, a mother–child unit was developed at ACCW based on the best interests of the child. With the support of Corrections Branch Headquarters, the ACCW health care team, correctional staff (both managers and frontline staff) and other provincial ministry personnel, it was decided ACCW could facilitate the return of mothers and babies to ACCW when recommended by BC Women’s Hospital and agreed to by the Ministry of Children and Family Development (MCFD), who had final authority over the placement of the child.
The decisions to place the mother and child together at the correctional facility were made by an interdisciplinary team consisting of the key staff from BC Women’s Hospital, ACCW health care, ACCW administration and the MCFD. If the mother was Indigenous, the pertinent Indigenous communities were consulted, when applicable. The mother and her family were included in all stages of this process. The support and services that Fir Square offered the mother before and after the birth fostered the mother’s confidence in parenting and in participating in the planning of her future and that of her baby. All checks and balances were put in place to ensure that ACCW was a safe and positive environment for the mothers and babies, with the cooperation of the mothers, other incarcerated women and correctional staff.
Incarcerated women who gave birth and who were deemed by MCFD able and willing to provide appropriate parental care were allowed to keep their infants in their care while in prison. During the initiative’s duration (2005–2007), 13 babies were born to incarcerated mothers, nine of whom lived in prison with their mothers and stayed there until their mother’s release. Eight babies were breastfed for the duration of their mother’s prison stay. Fifteen months was the longest stay of any infant in prison. The babies’ health and development was monitored by the community public health nurses, ACCW health care providers and MCFD social workers.
Release planning for the majority of the mothers and babies included placement at a residential supportive residence for women with substance use histories of the Fraser Health Authority, which took mothers and their young infants. The residential placement staff aimed to facilitate the transition of these women into the community.
Being involved in the initiative with BC Women’s Hospital had a profound positive effect on the women directly involved, the correctional staff and other incarcerated women, and the ministries and community agencies who partnered with ACCW.
Mother–child unit facilitates maternal involvement
Initially, other agencies and ministries were surprised and cautious regarding the proposal of the newborn babies returning to the facility with their mothers. The team at ACCW and BC Women’s Hospital took the time and facilitated many discussions and held meetings for all stakeholders to contribute to the program’s success.
Initially, the rights of the infant to be with the mother for attachment, bonding and breastfeeding was overshadowed for some by the feeling that this “privilege” should not be afforded to incarcerated mothers. As the initiative continued, the attitudes of many began to shift from cautious and guarded to comfortable and supportive. Community agencies were willing to provide supportive services to the children and mothers within the correctional facility. The collaboration reduced the need for ACCW to develop programs and services specific to the incarcerated population.
The mothers involved expressed great joy and were grateful that they could continue to breastfeed and nurture their babies at the correctional facility. They participated in parenting classes provided by a community agency through visits by the public health nurses and the MCFD worker. They also participated in health examinations by the ACCW physician to ensure the safety and health of their babies. Several of the mothers were permitted to go out into the community on escorted passes, both before and after the birth of their babies, to participate in various programs offered by community agencies that welcomed their participation.
Other women who did not have the opportunity to be with their children had to deal with the reminder of the pain they suffered as a result of being away from their own children. Seeing the babies at ACCW triggered feelings of loss, but a general feeling of hope permeated the entire population and the atmosphere at the facility was more positive in many ways. Incarcerated women wrote about their experiences as part of a prison participatory health research project, and their writing was later published in a book titled Arresting Hope.10
Seeing other ministries and agencies support this initiative had an impact on many of the incarcerated women. Most had very little trust in government agencies due to previous negative interactions. Seeing the agencies working together to ensure the babies stay with their mothers gave them a different perspective from which to view these groups. Some voiced a new interest to work with agencies to initiate contact with their own children with whom they had lost contact, or to work to improve their own lives to make a better life for their children.
For many, seeing the mothers and babies thrive at the facility and be released into the community together continued to reinforce the feeling that this initiative was not only the child’s right but also the right thing to do for the child.
Mother–child unit upheld by BC Supreme Court
In 2008, Brenda retired from ACCW and the BC Corrections Branch Headquarters shut down the prison mother–child unit. Amanda Inglis and Patricia Block, whose babies were born after the unit had closed, became appellants in a five-year legal case that led to a BC Supreme Court hearing in May 2013. During the women’s compelling testimony, Patricia told the court that there were as many as five different people caring for her daughter while they were separated. She tried to continue to breastfeed her baby while in prison, she said, but had difficulties in doing so.
At one point, her daughter’s foster mother stopped using the breast milk that Patricia had pumped because she worried it “wasn’t good milk.” Patricia had to inform the MCFD, who then ordered the foster mother to provide the breast milk to her baby. Patricia said that pumping milk in her prison cell for her newborn baby, who was then staying with relatives, gave new meaning to the phrase “crying over spilt milk.”
In December 2013, Honourable Judge Carol Ross ruled in Inglis v. British Columbia (Minister of Public Safety) that the cancellation of the mother–child unit infringed the Charter right to security of the person (section 7) of the mothers and babies affected by the decision, and that the infringements were not in accord with the principles of fundamental justice. The ruling also held that the cancellation constituted discrimination and violated section 15(1) of the Charter, the right to equality of the members of the affected groups, namely provincially incarcerated mothers who wished to have their baby remain with them while they serve their sentence and the babies of those mothers.
The judge directed the government of British Columbia to administer the Correction Act Regulation in relation to this issue in a manner consistent with the requirements of sections 7 and 15(1), and she gave six months to provide an opportunity for the government to correct the unconstitutionality of the present situation and comply with the Court’s direction.11
Guidelines developed to facilitate program adoption across Canada
The Collaborating Centre for Prison Health and Education (CCPHE) hosted a two-day working meeting in March 2014 at the University of British Columbia to generate best practice evidence-based guidelines to inform the implementation of mother–child units across Canada. Experts were invited to present during four panel discussions entitled “The Rights of the Child,” “The Correctional Context,” “Pathways and Programs” and “Evaluation.”
Thirty stakeholder organizations were invited to contribute to the writing of the guidelines by selecting delegate representative(s) to participate in the working meeting. Delegates included those from BC Corrections Branch, Correctional Service Canada, New Zealand Corrections and Women in2 Healing (formerly incarcerated mothers).
The CCPHE contracted Sarah Payne to write an initial guideline framework based on her analysis of the meeting proceedings. A “content analysis” method was used to ensure that all themes developing from the meeting data were captured in the emergent guidelines. As a final stage, international resources and research publications, which had been presented by experts as evidence during the working meeting, were reviewed.
The resulting Guidelines describe 16 guiding principles and best practices required for optimal child and maternal health inside a correctional facility, including the correctional context, pregnancy, birth, education, correctional and medical care, discharge planning and community partner engagement. Delegates from BC Corrections Branch and Correctional Service Canada, who attended the writing meeting, incorporated the Guidelines’ principles and best practices into their respective organizations’ policies and procedures.
Follow-up evaluations of the mother–child unit currently under way
The ACCW mother–child unit was established on the principle that babies should accompany their mothers back to the ACCW, which was supported by the 2013 BC Supreme Court ruling that deemed it unconstitutional to separate the two. Currently, the “new” BC provincial program and the federal program (as well as programs in the U.S.) are based on the principle that it is a privilege for the incarcerated mother rather than a right: incarcerated pregnant women have to submit an application and go through a difficult, stressful and protracted approval process.
Some infants now currently reside with their mothers in federal women’s correctional facilities across Canada. However, bringing babies to live with their mothers inside provincial correctional facilities has been slow, even though a refurbished mother–child unit opened in July 2014 at ACCW. More education and understanding about the cultural, epigenetic, legal and permanent health impacts of a decision to remove a baby at birth can help support maternal and infant health in prisons across Canada.
A 10-year follow-up evaluation of the ACCW mother–child unit that ran from 2005 to 2007 is currently under way. Through in-depth interviews with mothers whose infants lived at ACCW, this evaluation is exploring their experiences and the current health and social development of their children.
Each of the mothers interviewed to date have reported that the decision to have her baby live with her in prison transformed her life. Each woman attributed the quality and quantity of time that she spent with her baby in ACCW to making a positive long-term impact on the mother–child relationship, and each reported that she now has an exceptionally close relationship with her child. Each woman also spoke very affectionately about her child’s attributes, with kindness and a caring nature as foremost.
Notes
- Ronald R. Abrahams et al., “Rooming-in Compared with Standard Care for Newborns of Mothers Using Methadone or Heroin,” Canadian Family Physician 53:10 (October 2007), http://bit.ly/2k4K29I.
- Marian Knight and Emma Plugge, “The Outcomes of Pregnancy Among Imprisoned Women: A Systematic Review,” BJOG: An International Journal of Obstetrics and Gynaecology 112:11 (December 2005), doi.org/10.1111/j.1471-0528.2005.00749.x.
- Alison Cunningham and Linda Baker, Waiting for Mommy: Giving a Voice to the Hidden Victims of Imprisonment. London, ON: Centre for Children and Families in the Justice System, 2003.
- Helen Fair, “International Profile of Women’s Prisons,” World Prison Brief (February 7, 2008), http://bit.ly/2knx0BM.
- Kiran Bedi, It’s Always Possible: Transforming One of the Largest Prisons in the World. New Delhi: Stirling Paperbacks, 2006.
- Women’s Prison Association, “Mothers, Infants and Imprisonment: A National Look at Prison Nurseries and Community-Based Alternatives,” Institute on Women & Criminal Justice (May 2009), http://bit.ly/2hwPK0L.
- World Health Organization, “Infant and Young Child Feeding,” Fact Sheet (September 2016), http://bit.ly/1o6MEg8.
- Health Canada, “Nutrition for Healthy Term Infants: Recommendations from Birth to Six Months,” A joint statement of Health Canada, Canadian Paediatric Society, Dietitians of Canada, and Breastfeeding Committee for Canada (2013), http://bit.ly/LTH03C.
- Grace S. Marquis, “Breastfeeding and Its Impact on Child Psychosocial and Emotional Development,” Encyclopedia on Early Childhood Development (March 2008), http://bit.ly/1cESBkC.
- Ruth Elwood Martin, Mo Korchinski, Lyn Fels and Carl Leggo, eds., Arresting Hope: Women Taking Action in Prison Health Inside Out. Inanna Publications, 2014.
- Inglis v. British Columbia (Minister of Public Safety), 2013 BCSC 2309 (SC), H.M.J. Ross, http://bit.ly/2jiUVk0.
Dr. Ruth Elwood Martin is a Clinical Professor in UBC’s School of Population and Public Health and recipient of the 2015 Governor General’s Award in Commemoration of the Persons Case.
Brenda Tole is the former warden at the Alouette Correctional Centre for Women from the time it opened in 2004 until her retirement in 2008.
Download this article in PDF format.
Published on February 7, 2017
Timeline: Fifty Years of Women, Work and Family in Canada
While mothers in Canada have always played a central role in family life, there’s no question that the social, economic, cultural and environmental contexts that shape – and are shaped by – motherhood have evolved over time.
A growing share of mothers are managing paid work and family responsibilities compared with previous generations, and the dynamic relationships between women, work and family continue to evolve. To explore these relationships through a broader lens, we’ve created a 50-year timeline for Mother’s Day 2016 that explores some of the long-term trends over the past half century, including:
- An increase in women’s participation in the paid labour force, which has grown from 40% in 1968 to 82% in 2014 for those aged 25 to 54
- A growing share of “breadwinning” moms among single-earner couple families, which has steadily increased from 4% of earners in these families in 1976 to 21% in 2014
- A significant drop in the low-income rate among single mothers, which has fallen from 54% in 1976 to 21% in 2008
- A declining fertility rate, which stood at 3.94 women per children in 1959 during the peak of the baby boom, but has since dropped to 1.61 in 2011
- A continually rising average age of first-time mothers, up from 24.3 years of age in 1974 to 28.5 in 2011
- A greater amount of time mothers are spending with family, with women reporting 421 minutes (7 hours) per day with family in 2010, up from 403 minutes (6.7 hours) in 1986
This bilingual resource is a perpetual publication, and it will be updated periodically as new data emerges. Sign up for our monthly e-newsletter to find out about updates, as well as other news about publications, projects and initiatives from the Vanier Institute.
Enjoy our new timeline, and happy Mother’s Day to Canada’s 9.8 million moms!
Download the Fifty Years of Women, Work and Family in Canada timeline.
Language, Labels and “Lone Parents”
Victoria Bailey
Lone parent, single parent, one-parent family, independent parent, non-married parent, alone parent, autonomous parent: the words or terms used to identify, or self-identify, adults who parent independently are diverse and subjective, and they have evolved over the years. While our choice of labels may seem trivial, language is powerful and loaded – it shapes how we see the world and the people in it. These familial terms, and the respective ideas they aim to convey, are at best blurry. What can seem like a valid category to one person may be considered a stereotype by another, and these labels can carry stigma with them that has an impact on family well-being and identity – particularly for single mothers,1 who account for 8 in 10 single parents in Canada.
Many labels are used to categorize “lone parents”
Statistics Canada uses the term lone parent to identify “Mothers or fathers, with no married spouse or common-law partner present, living in a dwelling with one or more children.” They are not alone in this choice of terminology: the UK’s Office for National Statistics also utilizes the term lone parent/lone parent family, as does the UK government’s statistics website. The Australia Bureau of Statistics, meanwhile, uses the term one-parent family and Statistics New Zealand lists the term sole parent in its definitions of census family classifications but tends to defer to the same terminology as Australia in census information-related texts.
The United States Census Bureau uses a number of different terms in their definitions and reports; phrases including female householder, no husband present, single parent and lone parent are used to describe different family and/or household structures. In Engendering Motherhood, sociologist Martha McMahon frequently uses the term “unwed mother”; however, this text is now 20 years old and, once a commonly used term, “unwed mother” is now infrequently applied in either dialogue or in media content. To many people, the phrase may now seem dated, archaic and even tied to (and measured more by) religious doctrine.
In a sense, none of the terms commonly used to identify single mothers are satisfactory in their ability to capture family experiences, because they use deficit language. Lone mothers and sole mothers could suggest to some that these parents are “on their own,” without supports, while many of these parents may have rich networks of support that include family, friends, community organizations and even former partners. One-parent families suggests a similar isolation, whereas the child(ren) in these families may have two parents, even if the parents have ended their relationship. Whereas single parent/s, as with “unwed mother,” suggests a deviation from a married-parent norm, it is rare for a determining label of “married parent/s” to be used in conversation or in text unless focusing specifically on the topics of parenting and marriage.
Overall, the use of a variety of terms does seem like a more sensitive, considerate and inclusive approach that is more appreciative of complex family forms and provides options for identifying families. Whether intended or not, what the differing US Census Bureau terms and more modern, emerging phrases such as autonomous parent and independent parent do signify is that terminology related to being a single parent seems to be evolving and progressing in a way that attributes power to the parent’s choice of familial circumstance.
Terms have changed over time, as have family experiences and realities
The use of single-parent synonyms and their attributed meanings have developed over time, reflecting ever-changing family realities. According to Statistics Canada, the proportion of lone parents in our nation is not drastically different from what it was 100 years ago, and it was nearly as high in 1931 (11.9%) as it was in 1981 (12.7%). But what does differ, is the reason behind those numbers, that is, a modern-day choice of relationship status versus a latter-day result of circumstance, often related to mortality rates. As highlighted in the Statistics Canada report Enduring Diversity: Living Arrangements of Children in Canada over 100 Years of the Census:
… diverse family living arrangements were in many cases a result of the death of one or more family members. Death within the family – of siblings, of mothers during or following complications from childbirth, of fathers serving in war, for example – was a much more common experience for young children in the early 20th century than today. In 1921, about 1 in 11 (8.9%) children aged 15 and under had experienced the death of at least one parent, while 4.1% had experienced the death of both parents.
The researchers go on to point out, “In comparison, in 2011, less than 1% of children aged 0 to 14 lived in a lone-parent family in which the parent was widowed.”
Throughout Canada’s history, there have been diverse paths to parenting independently, such as through adoption, sperm/egg donation, surrogacy, in vitro fertilization (IVF) or through separation, divorce from, or death of, a partner – or there never having been a partner in terms of a relationship to begin with. To avoid reinforcing stereotypes, it is important in any discussion about single parents to acknowledge this diversity and avoid generalization or homogenization.
Family labels can have an impact on identities
The language and terms we use to identify family forms matter, as they can carry negative connotations and meaning. An example of this can be found in the 2011 Census definition of family, in which Statistics Canada included stepfamilies for the first time:
A couple family with children may be further classified as either an intact family in which all children are the biological and/or adopted children of both married spouses or of both common-law partners or a stepfamily with at least one biological or adopted child of only one married spouse or common-law partner and whose birth or adoption preceded the current relationship.
While counting stepfamilies is a positive step toward capturing diverse family forms, the decision to contrast this with the label “intact family” could suggest, to some, that families deviating from this status are not intact, that is, not whole or complete due to lack of a partner living under the same roof as a parent and their child.
Labels such as single mother or single parent may also not be terms some people feel comfortable with. For example, in an online article entitled “Single Mother Was Not a Title I Wanted to Own. A Year Later It Still Isn’t,” blogger Mavis King writes how both she, and other mothers, do not want to be labelled as “single mothers”:
The problem with being a “single mum”… is the negative connotations it can conjure. At their worst single mums are associated with welfare, dole-bludging, unkempt and unruly kids. The single mother is just keeping it together, just scraping by. She’s not a heroine, no she’s responsible for her plight. She should have known better, should have never married him, shouldn’t have had children. And what about the kids? She’s selfish, the kids won’t do well at school, they’re worse off than their friends.
However, some parents proudly take ownership of wording that communicates their self-sufficiency. On the Wealthy Single Mommy blog, for example, Emma Johnson writes, “I feel totally fine calling myself a single mom: I float my family financially and am the primary caretaker of my kids.”
Stigma related to “lone motherhood” can affect family well-being
Negative stereotypes about single mothers such as those described by King, that is, assumptions that single mothers are struggling and irresponsible, or that their children are worse off than others, are often fuelled and reinforced in the media. A recent post-graduate study I completed focused on the representation of single mothers in Canadian news media found that coverage typically followed three main trends: a negatively biased dichotomy of representation, homogenization of single mothers and application of the term “single mother” being connected to gender-related identification of familial status rather than relevance to article information.
These depictions bolster stereotypes that can have measurable consequences. For example, in a 2011 study into rental discrimination, single mothers were found to be more than 14% less likely to be granted a positive reply to rental inquiries than a (heterosexual) couple. Similarly, women who participated in a qualitative focus group for my dissertation research reported that the stigma of being labelled a single mother had acted as a barrier that prevented them from leaving negative situations, including statements such as, “I was more scared of being a single mom than of staying in an abusive relationship.”
Family labels gloss over diverse experiences
While many texts claim that being raised in a home by single parents may predispose children to negative outcomes, some research challenges the causal relationship between growing up in a single-parent family and detrimental outcomes. As researchers Don Kerr and Roderic Beaujot point out, “Studies that do not take into account the pre-existing difficulties of children and their families have a tendency to overstate the effect of growing up in a single-parent family.” There are many circumstances in which mothers have created healthier environments for themselves and their children precisely because they ended a negative relationship to become single mothers.
Often, it seems that resources, such as money, time and community supports (i.e. extended family, friends and other community members) have a more significant impact on child and parent experience and/or outcome than a parent’s relationship status. As Jon Bernardes states in Family Studies: An Introduction, “Whilst Queen Victoria was a single parent for many years, she is not thought of as a ‘problem parent.’”
However, what is perhaps most important to note is that children tend not to care about how the census categorizes their parents, nor do they tend to repeatedly quantify any kind of relationship status distinction when speaking about their parents. While they may initially share their familial status with friends – for example, “It’s just me and my dad” or “My dad doesn’t live with us” – there’s most likely an informal, colloquial tone to this statement. It’s highly unlikely that, once this personal information is shared, any future descriptions of an event or issue linked to their parent/s includes determining terminology such as “my single father” or “my lone parent mother.” They most likely simply say “my mom” or “my dad” or “my whomever” with a sense of confident, unconditional, personal belonging and attachment marking the initial, and perhaps most crucial, signifier in that type of statement: “my.”
1 This article frequently uses the terms “single mothers” and “single parents” for consistency, but as it discusses, there are many recognized and preferred terms in use.
Victoria Bailey is a freelance writer and a student of women’s studies. She lives and works in Calgary, Alberta.
Work–Family Conflict Among Single Parents in the Canadian Armed Forces
Alla Skomorovsky, PhD
The demands of military life can be particularly stressful for military families due to deployments, relocations, foreign residency, periodic family separations, risk of injury or death of the military member, and long and unpredictable duty hours.
Although military families can usually manage demands individually, research has shown that competing and intersecting demands leave some feeling overwhelmed. This can be particularly true for single parents in the Canadian Armed Forces (CAF), who often manage these multiple roles with fewer resources. This could help explain why enlisted single parents (men and women) have been shown in previous research to be less satisfied with military life than their married counterparts.
Work–family conflict occurs when demands in the work domain are incompatible with demands in the family domain. Despite growing evidence that work–family conflict could be a considerable problem in Canada’s military families, the number of studies examining this topic is relatively small. In a recent qualitative study, the majority of single CAF parents reported that they were able to balance work and family life, but they admitted it was a challenge, primarily because many single parents are often the sole caregivers and financial providers for their families. As one study participant put it,
“So far, the balance between my professional life and my personal life has been quite good. But it’s difficult of course when it’s just me – having to stay late, for example, and still having to work on my phone. I have to have a BlackBerry because I can’t stay late – not as late as I used to anyway. But pretty good, overall.”
Little research exists about work–family conflict in Canada’s military families
Single CAF parents may face multiple deployments and must deal with being separated from their children and not being able to care for them. Caregiver arrangements may be more complicated in these families, as, for example, the children may have to relocate to another city to live with grandparents when their mother or father leaves for a mission. In addition, single parents who experience frequent relocations may find it challenging to establish or re-establish local social networks, which are often a valuable source of support.
A few studies have suggested that single-parent military families have unique military life-related challenges and substantial work–family conflict, but there isn’t much research about this topic in a Canadian context. Director General Military Personnel Research and Analysis (DGMPRA) conducted a study to address this gap and explore the main concerns of single CAF parents. An electronic survey was distributed to a random sample of Regular Force CAF members who had children 19 years of age or younger and were single, divorced, separated or widowed. In total, the results were available for 552 single parents.
Single parents identified financial strain as a top concern; this is consistent with previous research showing that economic hardship is a leading cause of stress for single parents, both military and civilian. The second challenge for single parents was the worry about their child’s health and well-being. Although it has not been previously identified in research of civilian single parents, it is possible that this type of strain was high due to frequent parental absences related to deployment, training, unpredictable/inconsistent hours of work or overtime, common aspects of a military lifestyle. More than 60% of respondents identified financial strain and worry about health and well-being to be of considerable or extreme concern for them (see Figure 1). A large number of these parents (over 50%) were also concerned about dealing with adolescent years, doing the right thing for their children and their heavy demands and responsibilities.
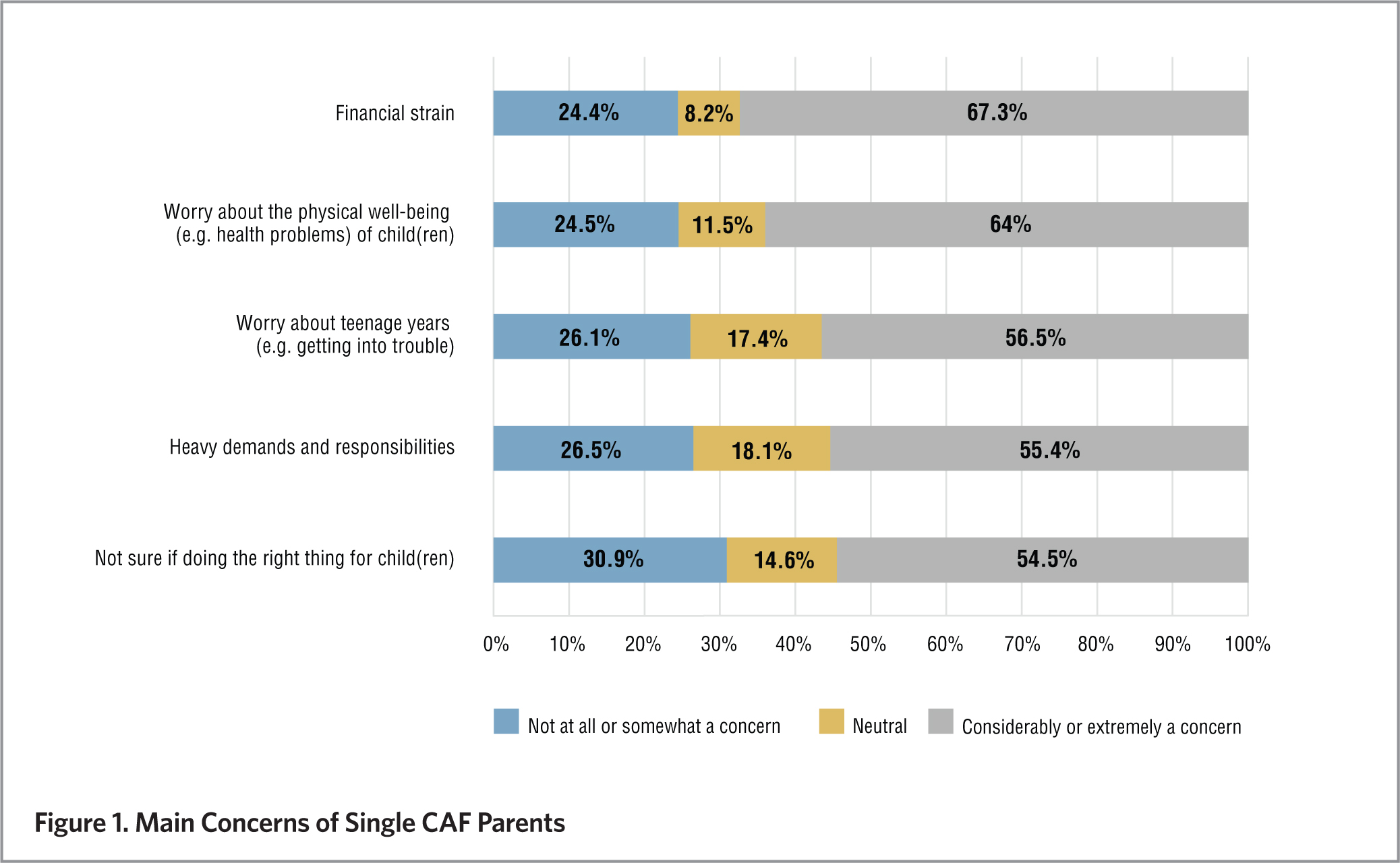
Managing parental and work responsibilities is not impossible, but it is hard
Single parents were asked to rate the extent to which their responsibilities as a service member and as a parent are in conflict. Most do not find it impossible to meet both parental and work responsibilities (see Figure 2). However, about 55% of respondents believe that it is not easy to be both a good parent and service member and feel divided between work and family responsibilities. About 44% of these parents believe it is hard to balance military and parental roles. This is consistent with previous research showing that single military parents are susceptible to experiencing work and family conflict.
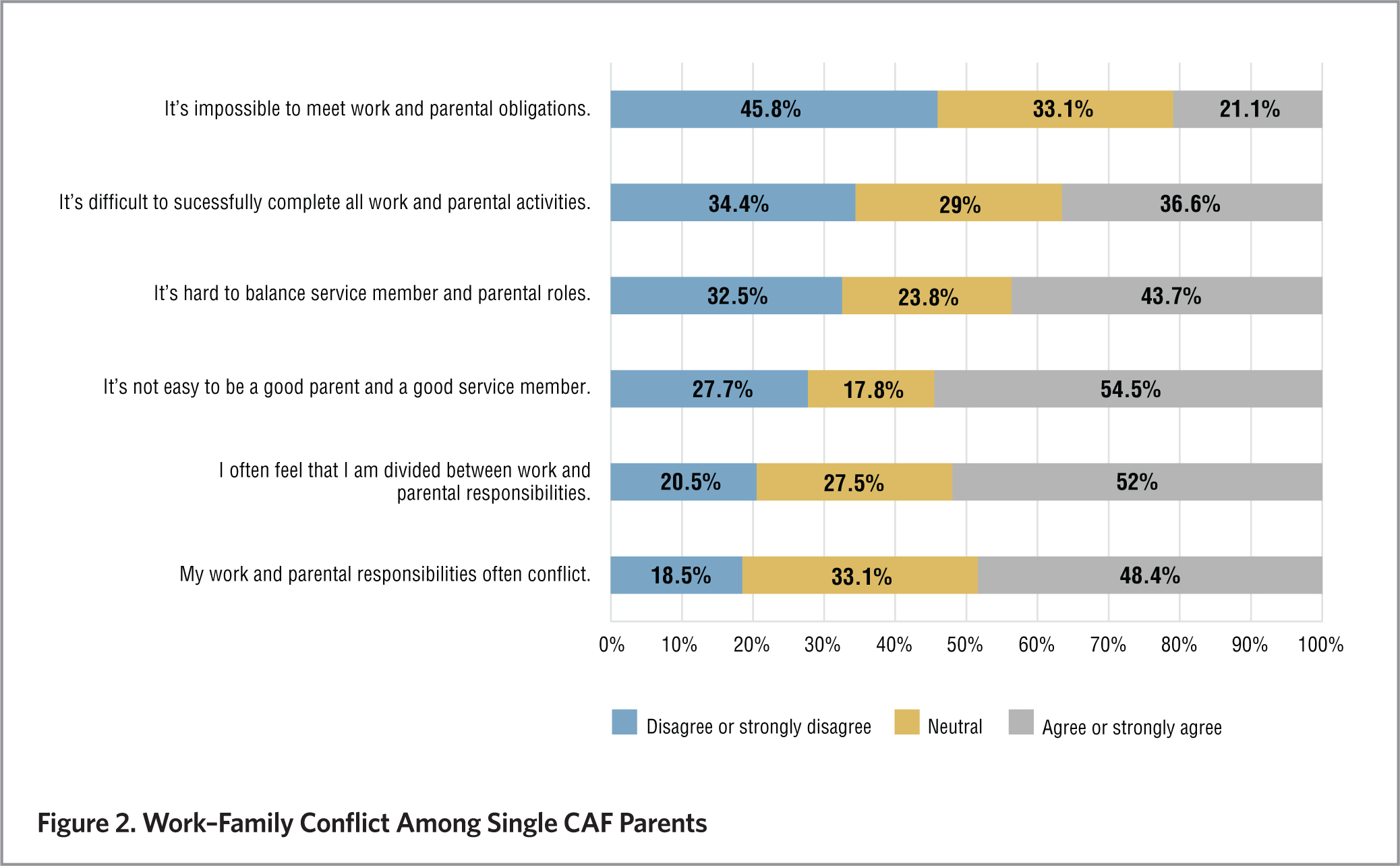
Further, participants were asked two questions about family life challenges due to occupational demands. When asked about the influence of work on family life, the vast majority of single military parents reported that work interferes with family life to at least some extent (see Figure 3). Approximately 70% of respondents noted that occupational demands sometimes conflicted with their family life, and 64% disclosed that they had missed family events due to occupational requirements.
In order to examine organizational support available to single parents in greater detail, single parents were asked whether they were aware of CAF programs and policies that could assist them in managing family and work demands. The results demonstrate that many single CAF parents are not aware of services available to them. For example, less than 10% of the participants mentioned that they were aware of Military Family Resource Centre services available to single military parents. This feeling was shared by a participant in the previously-mentioned qualitative study:
“Not everything is well advertised; you need to go and ask. If you are moving to the larger city, look for housing close to a [Military Family Resource Centre].”
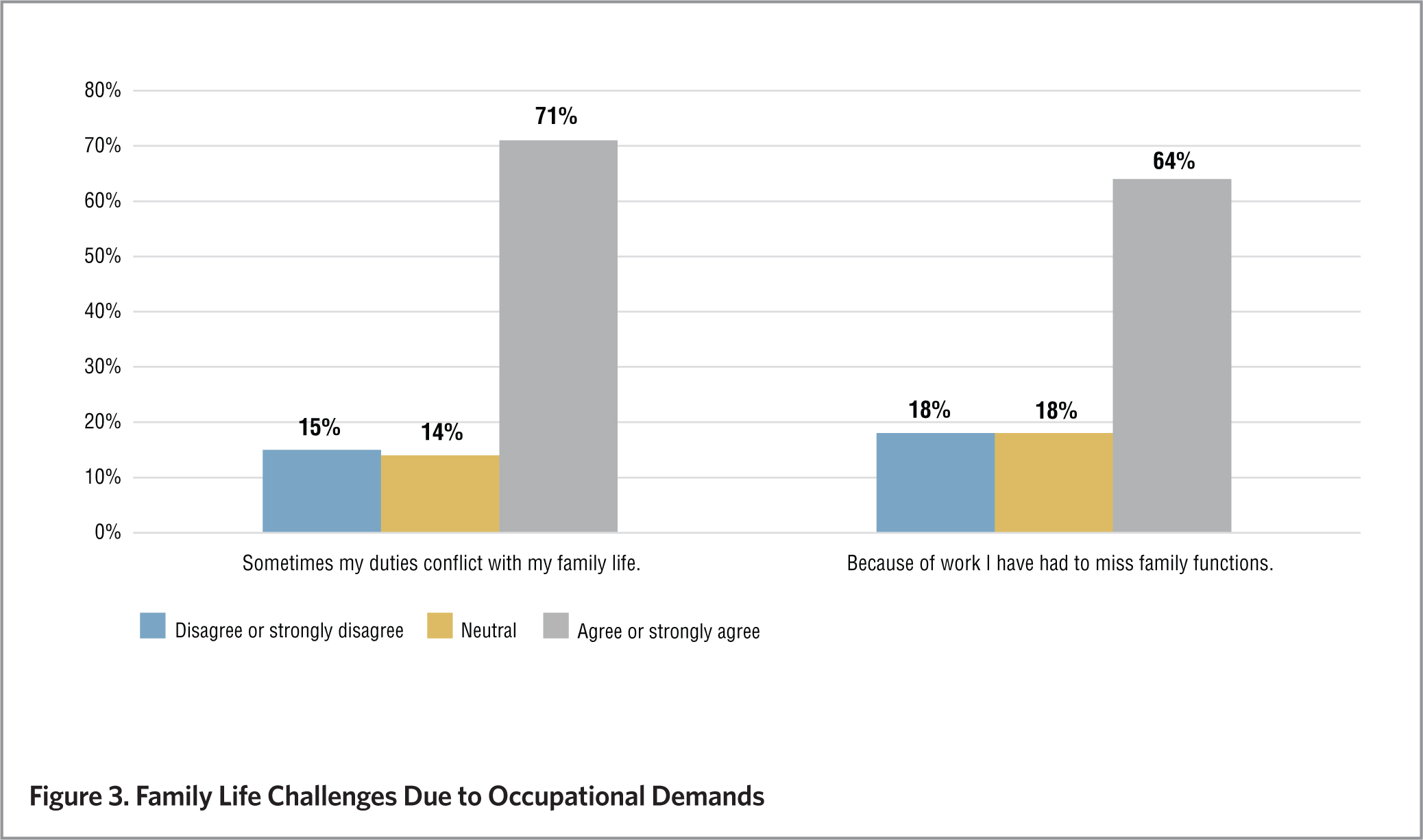
Single CAF parents would benefit from work–family supports and greater awareness
Many single CAF parents are thriving, but the work–family conflict remains a considerable concern for some. A qualitative study participant expressed:
“I’m mainly concerned that being in the Canadian Forces may throw something unexpected at me, where I will be left in a position to choose between my career or my children.”
Single CAF parents could benefit from an increased awareness of, and access to, family assistance programs (e.g., Family Care Plans) and other programs, including counselling services. Furthermore, increasing awareness among managers and leaders about the work–family conflict challenges of single CAF parents could foster a more flexible and accommodating work environment. Finally, the ability of these parents to manage work and family responsibilities could be enhanced by tailoring programs and services to single parents (e.g., support groups) in order to increase emotional and instrumental support.
Although this research examines the main challenges and work–family conflict among single-parent CAF families, this is only a first step toward a full understanding of their well-being and unique needs. To further address the current gaps in knowledge, DGMPRA has developed a comprehensive research program related to military families, collaborating extensively with academia (e.g., via Canadian Institute for Military and Veteran Health Research). This body of research seeks to enhance the lives of Canadian military personnel, Veterans and their families. Supporting families is codified in the Canadian Forces Family Covenant, which acknowledges the immutable relationship between the state of military families and the CAF operational capacity.
We recognize the important role families play in enabling the operational effectiveness of the Canadian Forces and we acknowledge the unique nature of military life. We honour the inherent resilience of families and we pay tribute to the sacrifices of families made in support of Canada…
Canadian Forces Family Covenant
Consistent with the Family Covenant, it is important to continue developing the expert knowledge necessary to care for these families and to find ways to best meet their unique needs and ensure their individual and family well-being.
Dr. Alla Skomorovsky is a research psychologist at Director General Military Personnel Research and Analysis (DGMPRA), where she is a leader of the Military Families Research team. She conducts quantitative and qualitative research in the areas of resilience, stress, coping, personality and well-being of military families.
Dr. Skomorovsky received the inaugural Colonel Russell Mann Award for her research on work–family conflict and well-being among CAF parents at Forum 2015 – an event hosted by the Canadian Institute for Military and Veteran Health Research.
This article can be downloaded in PDF format by clicking here.
Suggested Reading
T. Allen, D. Herst, E. Bruck and M. Sutton, “Consequences Associated with Work-to-Family Conflict: A Review and Agenda for Future Research,” Journal of Occupational Health Psychology, 5(2), 278–308 (2000).
G.L. Bowen, D.K. Orthner and L. Zimmerman, “Family Adaptation of Single Parents in the United States Army: An Empirical Analysis of Work Stressors and Adaptive Resources,” Family Relations, 42, 293–304 (1993).
A.L. Day and T. Chamberlain, “Committing to Your Work, Spouse, and Children: Implications for Work–Family Conflict,” Journal of Vocational Behavior, 68(1), 116–130 (2006).
A. Skomorovsky and A. Bullock, The Impact of Military Life on Single-Parent Military Families: Well-Being and Resilience (Director General Military Personnel Research and Analysis Technical Report DRDC-RDDC-2015-R099), Ottawa, ON: Defence Research and Development Canada (2015).
Modern Motherhood: The Unique Experiences of Women with Physical Disabilities

Lesley A. Tarasoff
There is very little research concerning pregnancy, labour, birth and motherhood among women with physical disabilities and women with disabilities more broadly. While most women face a variety of social and emotional pressures to have children, research has found that women with disabilities have a very different experience, as they are often pressured not to have children. Many of these girls and women experience “training against motherhood” as soon as they are diagnosed as having a disability. Despite these pressures, there are many women with physical disabilities who are also mothers. Although in Canada it is difficult to determine just how many women with physical or mobility-limiting disabilities are mothers, data from the United States suggests that they are becoming mothers at similar rates to women without disabilities.
As part of a long-term project, a diverse group of women with physical or mobility-limiting disabilities in the Greater Toronto Area have been interviewed about their experiences during the perinatal period – pregnancy, labour, birth and early motherhood. Drawing on other research studies and preliminary findings from this project, this article looks at some of the unique experiences of women with physical disabilities during the perinatal period.
While most women face a variety of social and emotional pressures to have children, research has found that women with disabilities are often pressured not to have children.
There are many misconceptions about women with physical disabilities, including the idea that they cannot or should not become mothers. Women with physical disabilities are often on the receiving end of disability and reproductive “microaggressions.” Initially conceptualized with regard to racial and ethnic minority groups, microaggressions refer to “the brief and commonplace, daily verbal, behavioral, and environmental indignities, whether intentional or unintentional, that communicate hostile, derogatory, or negative … slights and insults on the target person or group.” Disability or ableist microaggressions include things such as exclusion, messages of undesirability, messages of burden, assumptions, pity and astonishment (e.g., the realization that a person with a disability is capable of achievements).
For women with disabilities who are pregnant or who are mothers, these ableist beliefs and patterns of behaviour are often compounded with what some call reproductive microaggressions. These can be direct, such as denying privacy by asking when a woman will have a baby, or indirect, such as expressions of gratitude for having a “healthy child.” Underlying many reproductive microaggressions is reproductive privilege (i.e., the traditional idea or ideal of which women should be mothers [read: white, middle-class, heterosexual, women without physical disabilities]), together with the idea that motherhood is the most exalted form of identity for women.
Jane, one of the research project participants – a married and employed mother of two with a spinal cord injury – shared her thoughts about her perinatal experience. While it was positive overall, largely thanks to her strong advocacy skills and a great team of health care providers, she still experienced a number of negative social interactions commonly experienced by women with physical disabilities in the perinatal period. Sometimes these interactions were overtly discriminatory and negative, such as when a stranger on the sidewalk told her she “shouldn’t be allowed to have children.” Other times, the microaggressions were less explicit. Like many women with physical disabilities, Jane found that many people didn’t see pregnancy as a possibility for her or recognize her as being pregnant as they might have with other women. She often encountered subtle reactions of surprise (astonishment) to her pregnancy and status as a mother while in public spaces such as waiting rooms. Sometimes the microaggressions she described took the form of differential treatment, such as the time she was asked in a grocery store whether she had her daughter “naturally” – noting that it’s unlikely a mother without a disability would have been asked the same question.
Research suggests that women with physical or mobility-limiting disabilities are becoming mothers at similar rates to women without disabilities.
Microaggressions at the intersection of disability and reproduction can also take the form of denying identity or personality by asking a mother without disabilities “Is that your baby?” or of desexualizing women with disabilities through comments such as “I can’t believe you have a baby.” These comments were occasionally directed at Jane, who said that many people she encountered assumed that she had adopted. Microaggressions sometimes take on a patronizing form, such as when people say they feel “inspired” by women with disabilities who decide to have children. Finally, microaggressions also include assumptions of helplessness and infantilizing remarks directed at these mothers, such as asking “Do you need help with your baby?”
Despite the assumption that spinal cord-injured women are able to give birth only via Caesarean section, research reveals that they can have vaginal births. “Everyone still thinks that I had a C-section,” says Jane, acknowledging this misconception.
Indeed, a growing body of research indicates that many women with physical disabilities experience fertility no differently than their counterparts without disabilities and they are capable of becoming pregnant and experiencing vaginal delivery. Though limited, there is some research concerning the pregnancy outcomes of women with physical disabilities. Some of this research suggests that expectant mothers who have physical disabilities may experience common symptoms of pregnancy more severely, and that pregnancy can temporarily or permanently “alter the course” of the disability.
Perinatal outcomes among women with physical disabilities vary depending on the type and severity of their disability. “As much as I want to say that my pregnancy was the same as everyone else’s,” Jane says, “I do admit that there probably were higher risks of complications with mine to a certain degree.” For instance, she noted that her mobility worsened during the course of her pregnancy – a change that she says wasn’t fully recognized by care providers. Indeed, studies reveal that health care providers generally do not know a great deal about the interaction of pregnancy and disability. Jane cited an example of her nurses not knowing a lot about the different catheter options.
Likewise, many of the women with physical disabilities who were interviewed, including Jane, reported feeling frustrated with the lack of perinatal information available to them and often experienced feelings of isolation because it was difficult to find others to share their experiences with. “I found it very frustrating that there is so little research. So any question I had, nobody could give me an answer,” she says. “It was always like, ‘We don’t really know. We’re not really sure.’” In addition to informational barriers, many women with physical disabilities report encountering inaccessible care settings. Jane cited examples such as places with bathrooms or showers she couldn’t access or fit her wheelchair into.
Disabled or not, at one time or another, everybody needs assistance, and it is rare that someone really, truly raises a child single-handedly.
Exploring how women with physical disabilities experience the perinatal period will provoke an interrogation of the self, of what is “normal” and what accessibility is, as well as what independence looks like. Parents with disabilities, like all parents, are creative and adaptable. In many cases, formal resources and supports are not available or accessible, and so some parents with disabilities may rely on unconventional resources and other supports to fulfill their roles effectively. At one time or another, everybody needs assistance whether they have a disability or not, and it is rare that someone really, truly raises a child single-handedly.
Moreover, for some mothers with physical disabilities, becoming a parent takes focus away from their disability and places it on other aspects of their lives, such as the new bond between parent and child as well as the child’s imagination and creativity. As Jane puts it, “Becoming a mom is probably the best thing that I did because it totally lessened … my focus or other people’s focus on my disability. My parents ask way less about my own health; they ask more about the kids.”
In particular, Jane talked about how her physical inability to do certain activities with her young son has led to opportunities to bond and play with him in other ways:
“[My son] knows that I do all the creative stuff with him, so I do all the artwork… he kind of sees us [my husband and me] as having those different [roles] … I love doing imaginative things and I think that’s important for his growing and learning … so for me what’s really boosted my confidence in parenting is that I have that ability or that gift to do that with him and the daycare has commented that he’s such a really imaginative kid…”
A number of other mothers who were interviewed shared similar stories about their relationships with their children and talked about how becoming a mother enhanced their confidence.
Many of the mothers also worried about how their children might be treated in school when other children found out that their mother has a disability: “Kids can be mean… I don’t want people to make fun of him because of me.” One mother with a congenital condition that often limits her mobility, as well as causes hearing and vision problems, arthritis and chronic pain, noted, however, that she uses her disability as a learning opportunity for her young son: “I don’t want him to make fun of anybody. I am trying to tell him that everyone is different.”
The experiences of women with physical disabilities during the perinatal period, including their parenting experiences, provide learning opportunities for all families and their children. This ongoing research project will help to develop resources for women with physical disabilities and health care providers and shed light on some of the positive experiences that they have during the perinatal period. Listening to and documenting the stories and experiences of women like Jane will be integral to this process of providing support.
Lesley A. Tarasoff is a Ph.D. candidate in Public Health at the University of Toronto. She conducts research in the area of women’s sexual and reproductive health, with a focus on women with physical disabilities and sexual minority women. For more information about her research, visit www.latarasoff.com.
Learn more:
Lesley A. Tarasoff, “We Don’t Know. We’ve Never had Anybody Like You Before”: Barriers to Perinatal care for Women with Physical Disabilities,” Disability and Health Journal 10:3 (July 2017). Link: http://bit.ly/2fmk65C.
Lori E. Ross, Lesley A. Tarasoff, Abbie E. Goldberg and Corey E. Flanders, “Pregnant Plurisexual Women’s Sexual and Relationship Histories Across the Life Span: A Qualitative Study,” Journal of Bisexuality (August 11, 2017). Link: http://bit.ly/2wfhZaN.
Lesley A. Tarasoff, “Experiences of Women with Physical Disabilities during the Perinatal Period: A Review of the Literature and Recommendations to Improve Care,” Health Care for Women International 36:1 (July 2013). Link: http://bit.ly/2hqbiQE.
Update: In September 2017, a community report was published based on this research into the experiences of women with physical disabilities. “Becoming Mothers: Experiences of Mothers with Physical Disabilities in Ontario” is now available to download on Lesley’s website.
SOURCES
Judith Rogers, The Disabled Woman’s Guide to Pregnancy and Birth (New York: Demos Medical Publishing, 2006).
Corbett Joan O’Toole, “Sex, Disability and Motherhood: Access to Sexuality for Disabled Mothers,” Disability Studies Quarterly 22:4 (2002).
Lisa I. Iezzoni, Jun Yu, Amy J. Wint, Suzanne C. Smeltzer and Jeffrey L. Ecker, “Prevalence of Current Pregnancy Among US Women with and without Chronic Physical Disabilities,” Medical Care, 51:6 (June 2013).
Alette Coble-Temple, Ayoka Bell and Kayoko Yokoyama, The Experience of Microaggressions on Women with Disabilities: From Research to Practice and Reproductive Microaggressions and Women with Physical Limitations. Presentations at the American Psychological Association Annual Convention (August 2014).
Derald Wing Sue, Jennifer Bucceri, Annie I. Lin, Kevin L. Nadal and Gina C. Torino, “Racial Microaggressions and the Asian American Experience,” Cultural Diversity and Ethnic Minority Psychology, 13:1 (2007).
Ayoka K. Bell, Nothing About Us Without Us: A Qualitative Investigation of the Experiences of Being a Target of Ableist Microaggressions (2013 doctoral dissertation), retrieved from ProQuest Dissertations and Theses (dissertation/thesis number 3620204).
Heather Kuttai, Maternity Rolls: Pregnancy, Childbirth and Disability (Fernwood Publishing, 2010).
Caroline Signore, Catherine Y. Spong, Danuta Krotoski, Nancy L. Shinowara and Sean Blackwell, “Pregnancy in Women with Physical Disabilities,” Obstetrics & Gynecology, 117:4 (2011).
Suzanne C. Smeltzer and Nancy C. Sharts-Hopko, A Provider’s Guide for the Care of Women with Physical Disabilities and Chronic Health Conditions (2005).
Published on December 3, 2015
Updated on September 25, 2017
Modern Maternity Care in Canada
Cecilia Benoit
Georgina, a mother of Mi’kmaq heritage, is in the last stage of her pregnancy. Reluctantly, she is preparing to leave her home community of Port-aux-Basques, located on the southwestern tip of Newfoundland, to give birth in the only remaining maternity hospital in her health region, the Western Memorial Regional Hospital in Corner Brook, 220 kilometres away from her family and friends. Her chances of having a maternity doctor or midwife she knows attend her birth are slim to none, and there is a 30% chance that her baby will be delivered by Caesarean section.
Millennium Development Goal 5, to improve maternal health, is one of the United Nations Millennium Development Goals (MDGs). Of the eight MDGs, the least progress has been made toward the right of every woman to the best possible maternity care. Indigenous, poor and rural and remote women such as Georgina are especially compromised. While Canada made major strides throughout the 20th century to improve maternal health and build a universal maternity care system, many shortcomings remain, including but not limited to the medicalization of childbirth and inequitable access to maternity providers.
History of childbirth in Canada
Pregnancy and childbirth are significant life events in all cultures. In earlier times, midwives were the primary care providers. Care during pregnancy typically took place in the local community and birth occurred in the home.
Medicalization of maternity care in Canada, while significantly predating the development of the modern welfare state, became enshrined and solidified within the package of policies and regulations that accompanied the adoption of universal health care, known as “medicare,” which was implemented and formally adopted in 1972.
While Canada’s health care model is often referred to as a simple single payer health care system, funding and delivery of insured services are in fact much more complex. They involve federal and provincial/territorial governments, community services, private insurance companies and individuals.
Most physicians work in private practice, with their services paid from the provincial/territorial insurance plans. Funding for the insurance plans comes from the general revenues of the provinces/territories, with additional transfer payments from the federal government through the Canada Health and Social Transfer or, more recently, the Canada Health Transfer.
Under medicare, only physician-provided maternity care services were covered by the public health care system, which resulted in shifting the role of midwives (women) to medical doctors (mostly men). In the publicly funded health care system that was created, physicians also retained their right to remain private entrepreneurs, establishing their practices wherever they deemed appropriate.
The system created through medicare did not address the pre-existing disparity in the availability of physician services and solidified the hospital as the control centre of the maternity care system. Due to concerns about modesty and fear of contagion, it also excluded partners and other kin from participating in the age-old event of childbirth.
Modern childbirth in Canada
By the early 1980s, virtually all women across the country were delivering their babies in regional hospitals, attended by a maternity physician or obstetrician and assisted by obstetrical nurses. But these institutional changes left women lonely and new fathers sidelined. Research shows that women who have the support of a partner during labour require less pain relief and feel more positive about the birth. As research began to show the importance of healthy parent–child attachment, the health care system responded by allowing partners to be active participants in the birthing process. Partners today are present for the majority of births, taking on a greater role not only in these first moments of their children’s lives, but also with child rearing and household management in the years that follow.
Maternal deaths rose in Canada from 6 to 12 per 100,000 births between 1990 and 2013.
In 2013, UNICEF ranked Canada 22nd out of 29 high-income countries for infant mortality rates, with the rate substantially higher among Indigenous peoples.
Canada currently boasts the lowest maternal mortality rate in the American continent, reflecting improvements throughout the 20th century in women’s education, their nutrition, control of their fertility and universal coverage of physician services. Yet maternal deaths rose in Canada from 6 to 12 per 100,000 births between 1990 and 2013. By contrast, Japan and a number of European countries today have mortality rates half the Canadian rate or lower. Equally disconcerting, in 2013, UNICEF ranked Canada 22nd out of 29 high-income countries for infant mortality rates, with the rate substantially higher among Indigenous peoples.
In recent decades, the number of family doctors involved in maternity care delivery has significantly declined, as has the number of hospitals offering maternity care services. At the same time, the percentage of deliveries attended by obstetricians has increased substantially; for example, obstetricians currently attend 80% of hospital births in Ontario.
Caesarean section rates have also steadily increased, with the total national rate increasing from 17.6% in 1995 to 22.5% in 2001, and 27.3% in 2013 (see table below). The current rate of Caesarean section births ranges from a high of 32% in British Columbia and 31% in Newfoundland and Labrador to a low of 23.1% in Saskatchewan and 21.41% in Manitoba. According to the World Health Organization, Caesarean section rates below 10% indicate underuse of this life-saving procedure, while rates above 15% are deemed to show overuse. Overuse of Caesarean section has been linked to higher morbidity in mothers, including an increased risk for depression and post-traumatic stress, lower breastfeeding rates and a greater likelihood of future complications in pregnancy. Despite popular media images of maternal demand for Caesarean section, there is little evidence that the increase in the national rate in the last 20 years, and the even more surprising current cross-country variation, is based on mothers’ demand for a convenient pain-free birth – the so-called “too posh to push” argument.
Modern midwifery in Canada
Beginning with Ontario, British Columbia and Quebec in the 1990s, and spreading across most other regions since, midwives have received formal education and become regulated, and their services have been publicly funded. Yet the occupation still remains unregulated and unfunded in Newfoundland and Labrador, Yukon, Prince Edward Island and New Brunswick. Moreover, only 9% of births in Canada are currently attended by a midwife. While the percentage of midwife-attended births is higher in some regions (e.g., 19% in British Columbia), the demand outstrips the supply, with a substantial proportion of women in all parts of the country wanting access to a trained, publicly funded midwife but unable to find one.
Women with lower education, younger mothers, women without a partner and women living in rural and remote areas or socio-economically disadvantaged communities have the least access to publicly funded midwifery services. The Association of Ontario Midwives estimates that as many as 40% of women who want to see a midwife in Ontario are currently unable to find one, and women in other provinces are also experiencing frustration trying to find midwifery care. Following developments in Quebec and Manitoba, Ontario recently funded two free-standing, midwifery-led birth centres. Yet this option is not available for many non-Indigenous and Indigenous women, such as Georgina mentioned above, who instead experience loneliness, disconnection from their local maternity traditions and isolation from family; the overall result is “stressful births.”[ii]
Modern postpartum care in Canada
The length of time Canadian women spend in hospital following childbirth has decreased dramatically during the modern period, from a mean of five days in 1984–85 to just less than two days after vaginal delivery today. Hospital stays are costly; early hospital discharge for mothers and their newborns helps administrators control or reduce obstetrical care expenditures. For some women with strong support systems and access to publicly funded physician or midwifery services, early discharge from hospital is usually a welcomed occasion.
As in earlier times, family support can be crucial in the postpartum period. Fathers and/or partners across Canada, with the support of parental leave policies, are playing a much bigger role after childbirth than in previous generations – a shift in family roles that continues to this day. According to Statistics Canada, 31% of recent fathers across the country claimed or intended to take parental leave in 2013 – a significant increase from 3% in 2000. The rate is much higher in Quebec, particularly since the introduction of the Quebec Parental Insurance Plan (QPIP), which is the only plan in the country that specifically provides paternity leave. Since the introduction of QPIP in 2006, uptake has almost tripled, from 28% in 2005 to 83% in 2013.
But for women without these familial and formal options, the result can lead to negative health outcomes for themselves and their infants. Provincial and territorial health care systems cover a limited range of postnatal care services. At the federal level, this has traditionally been restricted to the provision of informational supports by the provinces and the publication of national guidelines for maternity and newborn care. In some regions, an optional home visit by either a public health nurse or a lay home visitor is still available, while in other regions, services following discharge from hospital have been reduced to a telephone call to a new mother from a public health nurse.
Privately delivered postnatal services have emerged to fill this care gap. There currently exist no published research studies on the for-profit postnatal services that currently exist in Canada. Postpartum doulas who advertise online often propose tangible, high-intensity supports such as newborn care, breast- and bottle-feeding support, child-minding services, meal preparation, household chores and so on. Unfortunately, relatively high out-of-pocket costs make these forms of support accessible only to those who are able to pay for them. Doulas who advertise online generally charge around $25 per hour, or anywhere from $100 to $1,000 for overnight or week-long package deals, respectively. Research studies in this emerging area of practice are needed to determine the scope of practice and outcomes for mothers and their families. There is currently no information available on user demographics, patterns of use or outcomes associated with these forms of commodified care, though such information would offer insight into the types and levels of unmet needs that exist.[iii]
The future of maternity care in Canada
As is clear from our history, midwives were the main maternity care providers in what is now Canada before the arrival of European settlers and up to the modern period. Midwives provided not only crucial technical care, but also social support to enhance the health and well-being of women and babies in homes and local communities. Modernization of maternity care involved the move from midwives and natural childbirth into the medicalization of childbirth, with obstetricians replacing family doctors as the maternity providers, and labour and delivery restricted to fewer and fewer hospitals. High Caesarean rates and the associated unnecessary morbidity for mothers is one outcome of this modern system of care. The return to midwifery and the integration of midwives into our health care system have thus far been insufficient, as midwives are too few in number, they are concentrated in urban centres and their services are not equally available in all provinces/territories.
As the country works toward achieving MDG 5, as families become more complex and partners become more involved in childbirth and child care, and as we have access to more research on how to increase positive health outcomes for mothers and newborns, the health care system will continue to evolve and adapt to ensure the availability and effectiveness of maternity care in our communities from coast to coast to coast.
Cecilia Benoit, PhD, is a Scientist at the Centre for Addictions Research of British Columbia, Professor in the Department of Sociology at the University of Victoria and former co-leader of the Women’s Health Research Network. She is also recipient of the 2016 Governor General’s Awards in Commemoration of the Persons Case.
Download this article in PDF format.
SOURCES
[i] Cecilia Benoit et al., “Medical Dominance and Neoliberalisation in Maternal Care Provision: The Evidence from Canada and Australia,” Social Science & Medicine, 71:3 (August 2010), accessed August 24, 2015. http://bit.ly/1Jv2r5j.
[ii] Cecilia Benoit et al., “Maternity Care as a Global Health Policy Issue,” The Palgrave International Handbook of Healthcare Policy and Governance, Ellen Kuhlmann, Robert H. Blank, Ivy Lynn Bourgeault and Claus Wendt (Eds.). Basingstoke: Palgrave, 2015. http://bit.ly/1NPii1r.
[iii] Cecilia Benoit et al., “Privatisation & Marketisation of Post-birth Care: The Hidden Cost for New Mothers,” International Journal for Equity in Health, 11:1 (October 2012). http://bit.ly/1ikd1BS.
Timeline: 50 Years of Families in Canada
Today’s society and today’s families would have been difficult to imagine, let alone understand, a half-century ago.
Families and family life have become increasingly diverse and complex, but families have always been the cornerstone of our society, the engine of our economy and at the centre of our hearts.
Learn about how families and family experiences in Canada have changed over the past 50 years with our new timeline!
Lone Mothers and Their Families in Canada: Diverse, Resilient and Strong
Mother’s Day is just around the corner, a time when children of all ages recognize and honour mothers, grandmothers and, increasingly, great-grandmothers! As we focus our attention on moms, many people worry about the prevalence of lone mothers and express concern about the well-being of their families.
“For many people, the term ‘lone mother’ brings to mind an image of a poor, struggling victim of sorts. They’re often seen as a single, growing group in crisis, toiling to raise children all on their own,” says Vanier Institute of the Family CEO Nora Spinks. “But this stereotype overlooks the diverse family experiences of lone mothers. This diversity, and the complexity of family life, is often lost in the statistics.”
“Of Canada’s 9.4 million families, only 16% lived in lone-parent families in 2011, with eight in 10 being led by women,” says Spinks. Many people feel that lone-parent families have been growing consistently over time. The truth, however, is more complex.
This belief is in part the result of looking only at trends since the 1960s, when the “traditional” family model with two married parents was at its peak. However, family structures fluctuate over time. Looking back further, lone-parent families were relatively common; the share of children living with a lone parent was 12% in 1931, similar to the 1981 rate of 13%.
While these numbers are close, the stories behind them differ because families faced different realities in these times. Many lone-parent families in the first half of the 20th century were in fact the result of mothers who died giving birth. The rate of children living in lone-parent families resulting from family death was eight in 10 in 1931. By the end of the century, it was only one in 10.
After the baby boom, a growing share of lone mothers were the result of separation and divorce, particularly following divorce law reform in 1968. This was just one of many changes for women in Canada during this period: women also gained greater capacity for family planning after the birth control pill emerged, and a growing number were pursuing higher education and joining the paid labour force, resulting in rising incomes.
This growth continues today, as the economic well-being of women improves. The incomes of lone mothers grew by 51% between 1998 and 2008 (compared to 13% among men). The income gap among lone parent families has shrunk: lone-parent families headed by women had incomes worth 53% of those headed by men in 1998, but 70% by 2008.
The prevalence of lone mothers, and lone-parent families in general, has always fluctuated over time. The reasons change, but the reality of ongoing change is constant. Families adapt and react to change, regardless of their form or the number of parents within.
The “lone mother” label often leads to another misperception: that these moms are without support. “Lone” suggests that these mothers are raising a family without any outside support (as does “sole” in the alternate label of “sole support mother”).
Often, these moms are not raising their children alone. Sometimes support comes from ex-partners. In 2011, 35% of separated or divorced parents said that decisions about their child(ren)’s health, religion/spirituality or education were made jointly or alternately. That same year, 9% said that their child(ren) live equally between their homes.
Support can come from other family members as well. In 2011, 8% of grandparents lived with their grandchildren, and one-third of these technically lived in “lone” parent households. “That’s 600,000 grandmas and grandpas in the family home, many of whom provide care and support to both generations,” says Spinks.
Multigenerational living is on the rise. It’s relatively common among immigrant and Aboriginal families. Shared living makes it easier to share costs, pool savings and provide care. Three-quarters of grandparents in lone-parent homes report some responsibility for household costs.
Many lone mothers may be in committed relationships with a partner who contributes to their family life, but choose to live in “living apart together” (LAT) couples. According to Statistics Canada, 8% of women aged 20 and over (1.9 million) are in LAT couples. However, we do not know how many of these are lone mothers.
Just as families are diverse, so are the forms of support they can provide and receive. Not all networks of care or forms of support are easy to capture with statistics. Lone mothers can be supported by friends or family members who offer help in ways such as child care; financial loans; living space; transportation; used toys, books or other goods; meals or groceries; and emotional support.
“Any portrait or discussion of modern lone mothers requires an open mind. One needs to understand that family life is diverse and complex, and families of all kinds are adaptable, strong and resilient. Myths and stereotypes about particular family types only lead to misunderstandings,” says Spinks. “That idea has guided the Vanier Institute of the Family since its founding 50 years ago, and will continue to as we study Canada’s families in the years ahead.”