
An overview of how technological change relates to inequalities within and between families
Topic: Disability
Issue Brief: Families, Disability, and Wellbeing in Canada

An overview of the wellbeing of families with disabilities in Canada
Researcher Spotlight: Margaret Campbell on Families, Disability, and Wellbeing

Margaret Campbell discusses her research on the wellbeing of families with disabilities in Canada.
Migration and Urbanization Trends and Family Wellbeing in Canada: A Focus on Disability and Indigenous Issues
A report prepared for Expert Group Meeting on megatrends and families
Disability, Work Mobility, and Support from “Family” (Families, Mobility, and Work)

Insights from lived experience on disability, mobility, and support.
In Brief: COVID-19 IMPACTS on Families Living with Disabilities
Vanier Institute’s In Brief Series: Mobilizing Research on Families in Canada
Diana Gerasimov
March 9, 2021
STUDIES:
Yang, F., K. Dorrance and N. Aitken. “The Changes in Health and Well-being of Canadians with Long-term Conditions or Disabilities Since the Start of the COVID-19 Pandemic,” StatCan COVID-19: Data to Insights for a Better Canada, Statistics Canada Catalogue no. 45-28-0001 (October 7, 2020). Link: http://bit.ly/3bXpkSh.
Arim, R., L. Findlay and D. Kohen. “The Impact of the COVID-19 Pandemic on Canadian Families of Children with Disabilities,” StatCan COVID-19: Data to Insights for a Better Canada, Statistics Canada Catalogue no. 45-28-0001 (August 27, 2020). Link: http://bit.ly/2QSNVxH.
Over the past year, the COVID-19 pandemic has negatively affected many Canadians’ physical and mental health,1 including limiting their access to services they may have otherwise reached out to for support. This can have a significant impact on those living with disabilities or long-term conditions, who are more likely to use health services on a regular basis and whose situation may be compounded by isolation and distance from familiar, informal social support.
In a recently published data from Statistics Canada, Canadians living with disabilities or long-term conditions who participated in a crowdsourced survey, from June to July 2020, reported declining health and mental health, as well as disruptions to health services. Variations in the general health of participants depend on the type of disability or long-term condition that individuals experience.
- 48% of participants living with disabilities or chronic conditions reported that their health was “somewhat worse” or “much worse” since before the pandemic.
- 64% of participants with cognitive conditions reported that their health had gotten “much” or “somewhat” worse compared with before the pandemic.
- 60% of individuals with mental health conditions reported that their overall health had gotten “much” or “somewhat” worse compared with before the pandemic.
- 48% of participants with hearing conditions reported their health to have stayed about the same.
- 73% of participants with mental-health related conditions reported “much worse” or “somewhat worse” mental health.
- 57% of participants with disabilities or chronic conditions self-rated their overall mental health as having declined since the beginning of the pandemic, while 36% reported that their mental health had not changed and 7% reported an improvement in their mental health (“somewhat better” or “much better”).
- 44% participants with hearing conditions reported consistent mental health since before the pandemic.
Families of children with disabilities
Another crowdsourced survey, which explored the experiences of parents of children living with disabilities, found that they were more likely to express concern for their children regarding their child’s mental health, anxiety and emotions, academic success and the impact of social isolation.
- 60% of parents of children with disabilities were concerned for their child’s mental health compared with 43% of parents with children without disabilities.
- 76% of parents of children with disabilities were very concerned about regulating their child’s anxiety and emotions, compared with 57% of parents of children without disabilities.
- 58% of parents of children with disabilities or long-term conditions were very concerned for their child’s academic success compared with 36% of parents of children without disabilities.
- 6 in 10 parents of children with disabilities were very concerned about social isolation compared with 5 in 10 parents of children without disabilities.
Diana Gerasimov holds a bachelor’s degree from Concordia University in Communication and Cultural Studies.
Note
- Learn more about the impact of COVID-19 on mental health in Family Finances and Mental Health During the COVID‑19 Pandemic and Do Adults in Couples Have Better Mental Health During the COVID‑19 Pandemic?
Families in Canada Interactive Timeline

Today’s society and today’s families would have been difficult to imagine, let alone understand, a half-century ago. Data shows that families and family life in Canada have become increasingly diverse and complex across generations – a reality highlighted when one looks at broader trends over time.
But even as families evolve, their impact over the years has remained constant. This is due to the many functions and roles they perform for individuals and communities alike – families are, have been and will continue to be the cornerstone of our society, the engine of our economy and at the centre of our hearts.
Learn about the evolution of families in Canada over the past half-century with our Families in Canada Interactive Timeline – a online resource from the Vanier Institute that highlights trends on diverse topics such as motherhood and fatherhood, family relationships, living arrangements, children and seniors, work–life, health and well-being, family care and much more.
View the Families in Canada Interactive Timeline.*
Full topic list:
- Motherhood
o Maternal age
o Fertility
o Labour force participation
o Education
o Stay-at-home moms
- Fatherhood
o Family relationships
o Employment
o Care and unpaid work
o Work–life
- Demographics
o Life expectancy
o Seniors and elders
o Children and youth
o Immigrant families
- Families and Households
o Family structure
o Family finances
o Household size
o Housing
- Health and Well-Being
o Babies and birth
o Health
o Life expectancy
o Death and dying
View all source information for all statistics in Families in Canada Interactive Timeline.
* Note: The timeline is accessible only via desktop computer and does not work on smartphones.
Published February 8, 2018
A Snapshot of Family Diversity in Canada (February 2018)
Download A Snapshot of Family Diversity in Canada (February 2018).
For more than 50 years, the Vanier Institute of the Family has monitored, studied and discussed trends in families and family life in Canada. From the beginning, the evidence has consistently made one thing clear: there is no single story to tell, because families are as diverse as the people who comprise them.
This has always been the case, whether one examines family structures, family identities, family living arrangements, family lifestyles, family experiences or whether one looks at the individual traits of family members, such as their ethnocultural background, immigration status, sexual orientation or their diverse abilities.
Building on our recent infographic, Family Diversity in Canada (2016 Census Update), our new Statistical Snapshot publication provides an expanded and more detailed portrait of modern families in Canada, as well as some of the trends that have shaped our vibrant and evolving family landscape over the years. Based on current data and trend analysis, this overview shows that diversity is, was and will continue to be a key characteristic of family life for generations to come – a reality that contributes to Canada’s dynamic and evolving society.
Highlights include:
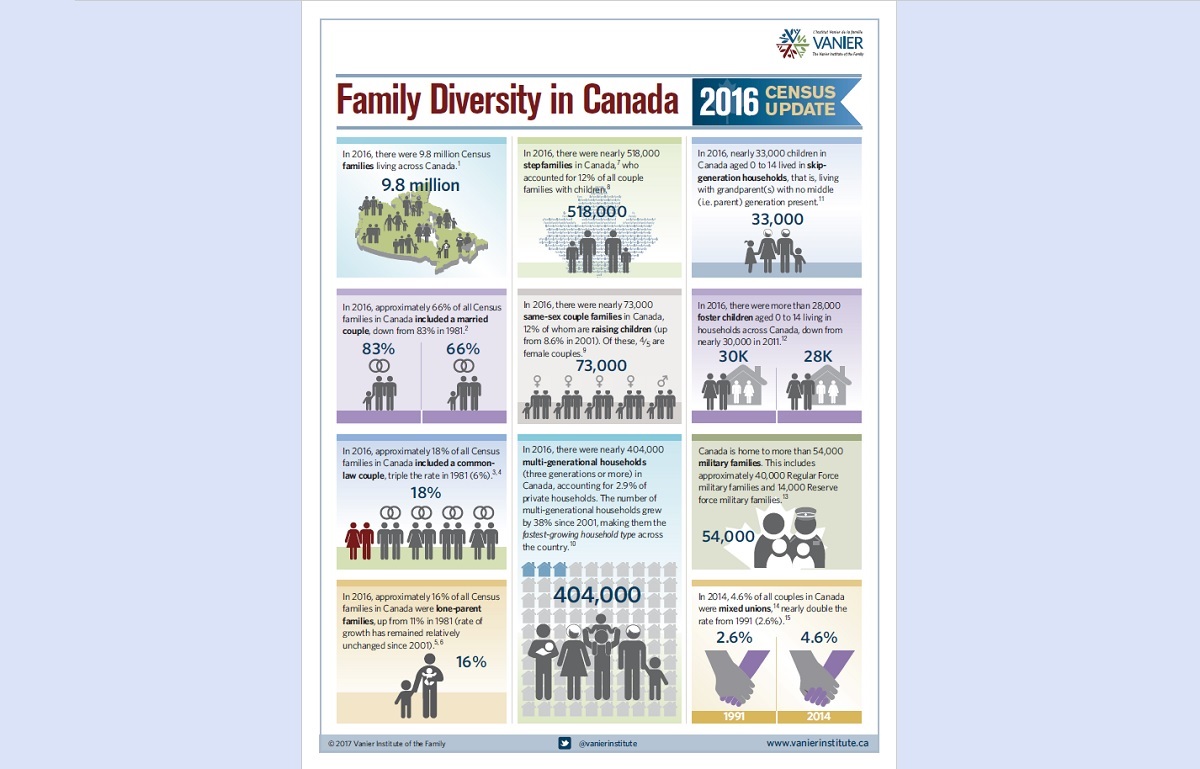
- According to Statistics Canada, there were 9.8 million Census families living across Canada in 2016.
- 66% of families in Canada include a married couple, 18% are living common-law and 16% are lone-parent families – diverse family structures that continuously evolve.
- Among Canada’s provinces, people in Quebec stand out with regard to couple/relationship formation, with a greater share living common-law than the rest of Canada (40% vs. 16%, respectively) and fewer married couples (60% vs. 84%, respectively) in 2016.
- In 2016, 1.7 million people in Canada reported having an Aboriginal identity: 58% First Nations, 35% Métis, 3.9% Inuk (Inuit), 1.4% other Aboriginal identity and 1.3% with more than one Aboriginal identity.
- In 2016, 22% of people in Canada reported that they were born outside the country – up from 16% in 1961.
- In 2016, more than 1 in 5 people in Canada (22%) reported belonging to a visible minority group, 3 in 10 of whom were born in Canada.
- 73,000 same-sex couples were counted in the 2016 Census, 12% of whom are raising children.
- In 2016, there were nearly 404,000 multi-generational households in Canada – the fastest-growing household type since 2001 (+38%).
- In 2011, 22% of Inuk (Inuit) grandparents, 14% of First Nations grandparents and 5% of Métis grandparents lived with their grandchildren, compared with 3.9% of among non-Indigenous grandparents.
- In 2014, 1 in 5 Canadians aged 25 to 64 reported living with at least one disability. Disability rates were higher for women (23%) than men (18%).
- More than one-quarter (27%) of Canadians surveyed in 2014 said religion is “very important” in their lives.
- One-quarter of Canadians reported “no religious affiliation” in the 2011 Census (most recent data available), up from 17% in 2001.
Download A Snapshot of Family Diversity in Canada (February 2018).
Health Care Experiences of Military Families of Children with Autism

Download this article in PDF format.
Heidi Cramm, Ph.D.
Military families in Canada are highly mobile, relocating three to four times more often than their civilian counterparts.1 This mobility has been found to complicate access to health care for these families, most of whom live off-base (85%, compared with only 20% in the mid-1990s) and rely on provincial and territorial civilian health care systems. This has an acute impact on the 8.2% of military families who have children with special needs, including those living with Autism Spectrum Disorder (ASD).2
Autism Spectrum Disorder (ASD) is a common neurodevelopmental disorder with an estimated prevalence of 1 in 68 children. While this condition primarily affects social communication, often making it difficult for people living with ASD to share enjoyment or emotional experiences with others, it has a range of symptoms and associated behaviours:
- Approximately 25% of people living with ASD are non-verbal, unable to use or respond to non-verbal communication (or are otherwise delayed in its use), such as pointing, gesturing and so forth, especially to indicate something of interest.
- People with ASD often have difficulties understanding abstract language/communication such as metaphors, sarcasm, colloquialisms and jokes.
- Repetitive behaviours, such as rocking, hand-flapping, finger movements and so forth, are common among people with ASD.
- People living with ASD are often highly sensitive to change, and they are “creatures of habit.”
- Most people with ASD have a range of sensory dysfunctions that vary widely (e.g., extreme sensitivities to noise, touch, smells, tastes, etc.) while many also exhibit a high pain threshold.
- Some children with ASD have exceptional abilities in music, visual and academic skills.
- In addition, up to 90% of children with ASD will have a co-existing medical and/or psycho-behavioural disorder, such as ADHD, anxiety, sleep disorders, feeding disorders, seizures, intellectual disability and gastro-intestinal disorders.
Early Intervention Supports Treatment for Children with ASD
Research suggests that early intervention is most impactful to the prognosis of ASD,3 and it can enhance the development of learning, communication and social skills for people living with the condition. Autism is typically diagnosed in early childhood, even as early as 18 to 24 months of age.
In many provinces, families experience long waiting times when seeking early diagnosis and/or intervention due to a “bottlenecking” of access to appropriate diagnostic centres – delays that can sometimes exceed two years.
Between 21% and 27% of military families do not have a family doctor, compared with 15% among the general population.4 Since many health services and treatments are accessed through family doctors, this discrepancy means that military families can have a harder time accessing services for children with special needs, including those with ASD. With each move, families who are moving toward the top of wait-lists for services find themselves back at the bottom.
Since many health services and treatments are accessed through family doctors, this discrepancy means that military families can have a harder time accessing services for children with special needs.
Exploring the Experiences of Military Families of Children with ASD
In a recent qualitative study, military families who have a child with ASD were interviewed to explore and describe their experiences navigating health care systems on behalf of their children.5
Many of these families reported that they had a hard time getting their child’s condition noticed, validated and medically diagnosed. Families generally found it difficult to get the assessment for ASD, and this delay in assessment and subsequent diagnosis meant that, for many, their access to intervention services was held up significantly.
One parent explained that their family experienced delays in accessing care for their son after moving because many of the programs available in their new community were for people living with autism who have a diagnosis. Since the family didn’t realize that they would need to have the diagnosis in hand when they sought care in their new neighbourhood, they went ahead and moved without having one, only to find that their son couldn’t access these programs as a result. Access to care for their child was delayed by months.
Difficulties accessing care can have an impact on family finances. Frustrated with wait-lists and the implications of delayed services for their child’s long-term development, many families opted instead to pay directly for private assessment services. One participant described making the decision to seek out private assessment and intervention because the wait-lists would exceed their posting tenure: “We paid privately… because the wait-list was too long. Once we had that diagnosis, [a community organization] put us on a wait-list for [Applied Behaviour Analysis] therapy. That wait-list is two years long. So we were never going to see the end of that wait-list either. So… we started paying privately for him.”
Frustrated with wait-lists and the implications of delayed services for their child’s long-term development, many families opted instead to pay directly for private assessment services.
At times, families waiting for care said they wound up moving again before their child’s name made it to the top of the local wait-list. For some families, service access was within sight, and then another posting forced them to move and start all over again. One participant shared that after waiting for some time for their child to get into a program, they finally received confirmation from their intervention team that the child would be able to start in September – which was of little help to them at that point, since they were going to be moving again in July.
With services varying widely from province to province (along with the corresponding eligibility and funding), some families reported consternation over losing services that they had previously had access to but were simply not available in their new location. One participant described this experience, “We realized the school [in the current province] didn’t offer the same things that they do in [the previous province]… there was nothing they could do…”
These variations also exist from region to region within the same province. For example, another participant described having to remove her child from a highly beneficial education program because they were moving, but then found they were unable to place him in a similar program in the new city because the program didn’t exist there (even though they were in the same province). Families in several other provinces described similar circumstances when moving interprovincially or intraprovincially.
Ongoing Pursuit of Health Care Affects Family Well-Being
While military families are highly resilient, difficulty accessing health care services for their children with ASD can have an impact on their own and their family’s well-being. Participants in the study commonly described frustration and confusion over the daunting tasks of sorting out how to get their children whatever services were possible. One participant described “bursting into tears” after finally getting to the top of a wait-list for intervention only to find the service did not meet expectations.
Some participants described having to draw on support from extended family to help care for their children. One participant said her parents retired and moved to the family’s current posting to assist because “they knew [our son] needed more help and we needed a break.” Others lamented the fact that extended family were too far away to really provide any assistance and were “just not able to be there.” Participants’ experiences with Military Family Resource Centres (MFRCs) were diverse, as the available services varied from base to base.
Parents often experienced strain on their relationships with their spouse or partner as their efforts to find caregiver supports and develop local networks can be complicated by training exercises, deployments and postings. As a result, hard choices are sometimes made related to whether or not a new posting, which comes with career opportunity, is feasible given the health care implications for the child with ASD.
Parents often experienced strain on their relationships with their spouse or partner as their efforts to find caregiver supports and develop local networks can be complicated by training exercises, deployments and postings.
Some participants described the Canadian Armed Forces (CAF) member making career decisions such as changing trades or requesting a specific posting for the benefit of the child, even though it could have an impact on their career trajectory and, by extension, the family as a whole. One participant said their family would consider living apart (i.e., imposed restriction) if it meant the child would receive the services needed, even though this would create a protracted separation that could have a significantly negative impact on the family as a whole.
In some military families, a civilian spouse may need to limit their involvement in the paid labour force to offset the caregiving requirements of the child. Such “trade-offs” are common in military families, with more than half (51%) of surveyed CAF spouses reporting that they have made some career sacrifices because of their partner’s military service, according to a 2009 study from the Director General Military Personnel Research and Analysis (DGMPRA). This limited workforce involvement can further constrain family finances that may be needed to pay for private services for their children. This can have a greater impact on dual-service families (families with two serving CAF members).
Military Families Express Desire for Navigation Support
Some military family members identified a few ways that could be considered to enhance the support for other military families who have children with ASD. Many expressed the desire to connect with other military families who are already at the new location to help map out options for how to access ASD-related services; some wanted this to be a formalized opportunity whereas others felt it would be important that it happen outside of official channels.
Many [families] expressed the desire to connect with other military families who are already at the new location to help map out options for how to access ASD-related services.
Opportunities to provide augmented and current information for families were also discussed, with some expressing a desire for a single point person who can help them navigate across school, community and health services. However, one participant indicated this type of formalized approach could result in parents receiving “filtered information” without any indication of how effective the services really are.
This qualitative study raised some important issues, but there is much left to learn. How might some of these opportunities be realized within existing formal and informal networks for incoming families? How could the disruptions and delays to health care access that military families report be reduced across provinces? What, if any, kinds of options might there be to offset the financial implications for parents when publicly funded services are absent or inaccessible? Are the differences for those who move within provinces similar to those who move across provinces? Exploring these questions through further research – with the insights and participation of families – will be key in supporting Canada’s diverse military families.
Dr. Heidi Cramm is the Interim Co-Scientific Director at the Canadian Institute for Military and Veteran Health Research (CIMVHR) and recipient of the 2016 Colonel Russell Mann Military Family Health Research Award.
Notes
- Heidi Cramm et al., “Making Military Families in Canada A Research Priority,” Journal of Military, Veteran and Family Health 1:2 (November 2015). Link: http://bit.ly/2zx46G1.
- Learn more with A Snapshot of Military and Veteran Families in Canada. Link: https://bit.ly/2fM3xmP.
- Geraldine Dawson, “Early Behavioral Intervention, Brain Plasticity, and the Prevention of Autism Spectrum Disorder,” Development and Psychopathology 20:03 (July 7, 2008). Link: https://bit.ly/2SWK2Lj.
- Nathan Battams, “A Snapshot of Military and Veteran Families in Canada,” Statistical Snapshots (November 2016). Link: https://bit.ly/2fM3xmP.
- Most of the families who participated in the study were married, and one-third of them had both parents serving in the Canadian Armed Forces (CAF). Most of the families represented serving members in the Regular Forces, primarily in the Army.
Infographic: Family Diversity in Canada (2016 Census Update)
Download the Family Diversity in Canada (2016 Census Update) infographic
The Vanier Institute of the Family has now been exploring families and family life in Canada for more than 50 years. Throughout this half-century of studying, discussing and engaging with families from coast to coast to coast, one thing has been clear from the outset: families in Canada are as diverse as the people who comprise them.
This has always been the case, whether one examines family structures, family identities, family living arrangements, family lifestyles, family experiences or whether one looks at the individual traits of family members such as their ethnocultural background, immigration status, sexual orientation or their diverse abilities.
These parents, children, grandparents, great-grandparents, aunts, uncles, siblings, cousins, friends and neighbours all make unique and valuable contributions to our lives, our workplaces and our communities. As former Governor General of Canada, His Excellency The Right Honourable David Johnston, said at the Families in Canada Conference 2015, “Families, no matter their background or their makeup, bring new and special patterns to our diverse Canadian tapestry.”
Using new data from the 2016 Census, the Vanier Institute has published an infographic on family diversity in Canada.
Highlights include:
- 66% of families in Canada include a married couple, 18% are living common-law, and 16% are lone-parent families – diverse family structures that continuously evolve.
- 518,000 stepfamilies live across the country, accounting for 12% of couples with children under age 25.
- 404,000 households in Canada are multi-generational,1 and nearly 33,000 children live in skip-generation households.2
- 1.7M people in Canada reported having an Aboriginal identity (58.4% First Nations, 35.1% Métis, 3.9% Inuit, 1.4% other Aboriginal identity, 1.3% more than one Aboriginal identity).
- 360,000 couples in Canada are mixed unions,3 accounting for 4.6% of all married and common-law couples.
- 73,000 same-sex couples were counted in the 2016 Census, 12% of whom are raising children.
- 54,000 military families live in Canada, including 40,000 Regular Force military families and 14,000 Reserve force military families.
Download the Family Diversity in Canada (2016 Census Update) infographic.
This bilingual resource is a perpetual publication, and will be updated periodically as new data emerges (older versions are available upon request). Sign up for our monthly e-newsletter to find out about updates, as well as other news about publications, projects and initiatives from the Vanier Institute.
Notes
- Containing three or more generations.
- Living with grandparent(s) with no middle (i.e. parent) generation present.
- Statistics Canada defines a mixed union as “a couple in which one spouse or partner belongs to a visible minority group and the other does not, as well as a couple in which the two spouses or partners belong to different visible minority groups.” Link: http://bit.ly/2tZvrSr.
A Snapshot of Workplace Mental Health in Canada

At some point in our lives, we are all affected by mental illness, whether through personal experience or that of a family member, friend, neighbour or colleague. Mental health conditions can have a significant impact on individuals, but they can also “trickle up” to have a detrimental effect on workplaces, communities, the economy and society at large – no one remains untouched. It is therefore vital that support for mental health be multi-faceted and every bit as prevalent as the conditions it seeks to address.
Stigma remains a major barrier to care for those living with a mental illness, many of whom are receiving, and benefiting from, care and support from their families.
This edition of the Vanier Institute of the Family Statistical Snapshots series explores mental health, families and work – three key parts of our lives that intersect and interact in complex ways that affect our well-being.
Highlights include:
- 4 in 10 Canadians have a family member with a mental health problem.
- At least 500,000 employed Canadians are unable to work due to mental health problems in any given week.
- Mental illness accounts for an estimated 30% of all disability claims and 70% of disability costs.
- Stigma remains an issue, with 1 in 5 surveyed Canadian employees saying they believe that whether or not someone becomes mentally ill is “fully within their control.”
- 4 in 10 surveyed Canadian employees say they would not tell their manager if they were experiencing a mental health problem.
- More than 7 in 10 Canadians who are affected by a family member’s mental health problem provided care to them, and 68% say they are not embarrassed about their family member’s mental health condition.
Download A Snapshot of Workplace Mental Health from the Vanier Institute of the Family.
Public Policy Brief – Flex: From a Privilege to a Right
Sara MacNaull
Working family members are multi-taskers, managing a variety of responsibilities at home, at work and in their communities. While family members demonstrate a great deal of adaptability in managing multiple roles, they benefit from workplaces that are respectful of their lives outside of work and responsive to their requests for flexibility and autonomy.
Workplace flexibility continues to be a topic of great interest to individuals, families, employers and policy makers. There are many approaches to creating flexible work environments, including modifications, adaptations and accommodations that impact when, where and how work gets done.
Workplace flexibility: A win-win-win strategy
Families are not the only ones who benefit from workplace flexibility as family members strive to effectively manage their multiple roles. Employers are embracing workplace flexibility as a key lever to attract and retain top talent in a competitive job market. Society benefits by having a stable workforce and an economy fuelled by organizations operating at peak performance.
Recently the Prime Minister of Canada identified workplace flexibility as a “top priority” in the mandate letter to the Minister of Employment, Workforce Development and Labour. In particular, the Minister was instructed to:
Work with the Minister of Families, Children and Social Development to fulfill our commitments to provide more generous and flexible leave for caregivers and more flexible parental leave.
… and to
Amend the Canada Labour Code to allow workers to formally request flexible work arrangements from their employers and consult with provinces and territories on the implementation of similar changes in provincially regulated sectors.
The proposed amendments to the Labour Code would mean that employees would be given the legal right to formally request flexible work arrangements from their employers.
Currently, in Canada there is no formal, legal mechanism for employees to request flex, and supervisors/managers are not legally required to consider such requests – the response is at the discretion of the employer. The right to request flex is considered by some to be a privilege for employees, and depends on the supervisor/manager’s personal perspective. Responses to requests are shaped by the culture of their organization. Right-to-request-flex legislation would change this by formalizing and normalizing this process while ensuring that employers justify why they refuse to grant the request, should they need to do so.
The Vanier Institute recently studied workplace flexibility in a benchmarking initiative that included a survey of employers and HR professionals. This survey found that employers offering flex is no longer considered optional, and is in fact key to attracting and retaining top talent in today’s competitive labour market. Many participants in the study also said that flex is already a right in their organization, as opposed to an employee privilege.
Flex is already a right elsewhere
Countries such as Australia and the U.K., as well as parts of the U.S., have implemented the right to request flex in their respective employment/labour legislations and/or regulations. However, eligibility requirements vary and, depending on the jurisdiction, it may not be available to all employees.
In Australia, the right to request flexible work arrangements (FWAs) was introduced through the Fair Work Act 2009, which provides employees who meet the eligibility requirements the legal right to request flexible work. Eligible employees include those:
- Who are parents or who have the responsibility to care for a child who is school-aged or younger
- With caregiving responsibilities (as defined by the Carer Recognition Act 2010)
- With a disability
- Who are aged 55 years and up
- Who are experiencing family violence or caring for someone who is experiencing family violence
- Who have worked for the employer for at least one year (though long-term casual employees may also be eligible)
In the U.K., the right to request flex was extended to all employees in 2014. Previously, this right had been limited to parents and carers, similar to some of the eligibility requirements in Australia.
In the U.S., eligibility requirements vary depending on the legislation within a particular jurisdiction. For example, employees within the state of Vermont were granted the right to request flex in 2014, the same year in which both the city of San Francisco employees and all federal U.S. employees were granted such a right.
Right to request differs from right to flex
In Australia and the U.K., the employer must provide, in writing, specific reasons for refusing a request for flex. The refusal must be due to reasonable business grounds, such as extra costs to the employer; significant loss in productivity, quality or performance; resulting inability to meet customer demands; or inability to reorganize work among other staff members.
While details of the pending right to request flex legislation are not public as of publication date, measures to facilitate flexible work could provide families with further support as they strive to manage their various responsibilities, commitments and obligations. For families, this means that work–life quality may be improved by having the time and energy to care for others and care for oneself while remaining a productive and committed employee.
Alternative work arrangements (AWAs) are temporary arrangements that differ from the norm within an organization (i.e. standard “9-to-5” workdays) and are case-by-case “one-offs” tailored to an employee’s short-term needs. These arrangements focus on the employee’s time in the office. Examples may include a phased return from maternity or parental leave for a pre-defined period of time or an adjustment to start and end times during the recovery period following an illness or injury.
Flexible work arrangements (FWAs) allow employees more flexibility and autonomy around when, where and how works gets done. FWAs help employees manage their multiple roles inside and outside the office. Though some employees may find it daunting to ask their supervisors for flex, as it may be perceived as an employee privilege, for many families it’s a necessity in order for them to manage the everyday needs of family. Examples of FWAs include remote work, compressed work weeks, job sharing and flex hours.
Customized work arrangements (CWAs) are individualized and personalized work arrangements that tailor when, where and how work gets done. Unlike AWAs and FWAs, these arrangements are fluid, extend over long periods or are modified as circumstances change. Employees are evaluated on output and productivity through a results-based approach, rather than a “clock-in/clock-out” approach focused on time spent physically present in the workplace. Examples include Mass Career CustomizationTM, for example, workload dial-up or dial-down, depending on an employee’s situation.
Sara MacNaull is Program Director at the Vanier Institute of the Family and is currently working toward earning the Work–Life Certified Professional designation.
This article can be downloaded in PDF format here.
Infographic: Family Diversity in Canada 2016
International Day of Families is approaching on May 15, a special day to recognize the importance of family to communities across the globe. Parents, children, grandparents, great-grandparents, aunts, uncles, siblings, cousins and the friends and neighbours we care for (and who care for us) all make unique and valuable contributions to our lives, our workplaces and our communities.
As we reflect on Canada’s 9.9 million families, one thing that’s clear is that there’s no such thing as a cookie-cutter family. Families are as diverse and unique as the people who comprise them, and they are all an essential part of Canada’s family landscape.
For this year’s International Day of Families, we’ve created an infographic providing a “snapshot” of modern families in Canada that highlights some of the many ways families are diverse:
- 67% of families in Canada are married-couple families, 17% are living common-law, and 16% are lone-parent families – diverse family structures that continuously evolve
- 464,000 stepfamilies live across the country, accounting for 13% of couples with children
- 363,000 households contain three or more generations, and there are also approximately 53,000 “skip-generation” homes (children and grandparents with no middle generation present)
- 1.4 million people in Canada report having an Aboriginal identity (61% First Nations, 32% Métis, 4.2% Inuit, 1.9% other Aboriginal identity, 0.8% more than one Aboriginal identity)
- 360,000 couples in Canada are mixed unions,* accounting for 4.6% of all married and common-law couples
- 65,000 same-sex couples were counted in the 2011 Census, 9.4% of whom are raising children
- 68,000 people in Canada are in the CAF Regular Forces, half of whom have children under 18
As His Excellency The Right Honourable David Johnston, Governor General of Canada, expressed at the Families in Canada Conference 2015, “Families, no matter their background or their makeup, bring new and special patterns to our diverse Canadian tapestry.” Join us as we recognize and celebrate family diversity, from coast to coast to coast.
Download the Family Diversity in Canada 2016 infographic.
* Statistics Canada defines a mixed union as “a couple in which one spouse or partner belongs to a visible minority group and the other does not, as well as a couple in which the two spouses or partners belong to different visible minority groups.”
Modern Motherhood: The Unique Experiences of Women with Physical Disabilities

Lesley A. Tarasoff
There is very little research concerning pregnancy, labour, birth and motherhood among women with physical disabilities and women with disabilities more broadly. While most women face a variety of social and emotional pressures to have children, research has found that women with disabilities have a very different experience, as they are often pressured not to have children. Many of these girls and women experience “training against motherhood” as soon as they are diagnosed as having a disability. Despite these pressures, there are many women with physical disabilities who are also mothers. Although in Canada it is difficult to determine just how many women with physical or mobility-limiting disabilities are mothers, data from the United States suggests that they are becoming mothers at similar rates to women without disabilities.
As part of a long-term project, a diverse group of women with physical or mobility-limiting disabilities in the Greater Toronto Area have been interviewed about their experiences during the perinatal period – pregnancy, labour, birth and early motherhood. Drawing on other research studies and preliminary findings from this project, this article looks at some of the unique experiences of women with physical disabilities during the perinatal period.
While most women face a variety of social and emotional pressures to have children, research has found that women with disabilities are often pressured not to have children.
There are many misconceptions about women with physical disabilities, including the idea that they cannot or should not become mothers. Women with physical disabilities are often on the receiving end of disability and reproductive “microaggressions.” Initially conceptualized with regard to racial and ethnic minority groups, microaggressions refer to “the brief and commonplace, daily verbal, behavioral, and environmental indignities, whether intentional or unintentional, that communicate hostile, derogatory, or negative … slights and insults on the target person or group.” Disability or ableist microaggressions include things such as exclusion, messages of undesirability, messages of burden, assumptions, pity and astonishment (e.g., the realization that a person with a disability is capable of achievements).
For women with disabilities who are pregnant or who are mothers, these ableist beliefs and patterns of behaviour are often compounded with what some call reproductive microaggressions. These can be direct, such as denying privacy by asking when a woman will have a baby, or indirect, such as expressions of gratitude for having a “healthy child.” Underlying many reproductive microaggressions is reproductive privilege (i.e., the traditional idea or ideal of which women should be mothers [read: white, middle-class, heterosexual, women without physical disabilities]), together with the idea that motherhood is the most exalted form of identity for women.
Jane, one of the research project participants – a married and employed mother of two with a spinal cord injury – shared her thoughts about her perinatal experience. While it was positive overall, largely thanks to her strong advocacy skills and a great team of health care providers, she still experienced a number of negative social interactions commonly experienced by women with physical disabilities in the perinatal period. Sometimes these interactions were overtly discriminatory and negative, such as when a stranger on the sidewalk told her she “shouldn’t be allowed to have children.” Other times, the microaggressions were less explicit. Like many women with physical disabilities, Jane found that many people didn’t see pregnancy as a possibility for her or recognize her as being pregnant as they might have with other women. She often encountered subtle reactions of surprise (astonishment) to her pregnancy and status as a mother while in public spaces such as waiting rooms. Sometimes the microaggressions she described took the form of differential treatment, such as the time she was asked in a grocery store whether she had her daughter “naturally” – noting that it’s unlikely a mother without a disability would have been asked the same question.
Research suggests that women with physical or mobility-limiting disabilities are becoming mothers at similar rates to women without disabilities.
Microaggressions at the intersection of disability and reproduction can also take the form of denying identity or personality by asking a mother without disabilities “Is that your baby?” or of desexualizing women with disabilities through comments such as “I can’t believe you have a baby.” These comments were occasionally directed at Jane, who said that many people she encountered assumed that she had adopted. Microaggressions sometimes take on a patronizing form, such as when people say they feel “inspired” by women with disabilities who decide to have children. Finally, microaggressions also include assumptions of helplessness and infantilizing remarks directed at these mothers, such as asking “Do you need help with your baby?”
Despite the assumption that spinal cord-injured women are able to give birth only via Caesarean section, research reveals that they can have vaginal births. “Everyone still thinks that I had a C-section,” says Jane, acknowledging this misconception.
Indeed, a growing body of research indicates that many women with physical disabilities experience fertility no differently than their counterparts without disabilities and they are capable of becoming pregnant and experiencing vaginal delivery. Though limited, there is some research concerning the pregnancy outcomes of women with physical disabilities. Some of this research suggests that expectant mothers who have physical disabilities may experience common symptoms of pregnancy more severely, and that pregnancy can temporarily or permanently “alter the course” of the disability.
Perinatal outcomes among women with physical disabilities vary depending on the type and severity of their disability. “As much as I want to say that my pregnancy was the same as everyone else’s,” Jane says, “I do admit that there probably were higher risks of complications with mine to a certain degree.” For instance, she noted that her mobility worsened during the course of her pregnancy – a change that she says wasn’t fully recognized by care providers. Indeed, studies reveal that health care providers generally do not know a great deal about the interaction of pregnancy and disability. Jane cited an example of her nurses not knowing a lot about the different catheter options.
Likewise, many of the women with physical disabilities who were interviewed, including Jane, reported feeling frustrated with the lack of perinatal information available to them and often experienced feelings of isolation because it was difficult to find others to share their experiences with. “I found it very frustrating that there is so little research. So any question I had, nobody could give me an answer,” she says. “It was always like, ‘We don’t really know. We’re not really sure.’” In addition to informational barriers, many women with physical disabilities report encountering inaccessible care settings. Jane cited examples such as places with bathrooms or showers she couldn’t access or fit her wheelchair into.
Disabled or not, at one time or another, everybody needs assistance, and it is rare that someone really, truly raises a child single-handedly.
Exploring how women with physical disabilities experience the perinatal period will provoke an interrogation of the self, of what is “normal” and what accessibility is, as well as what independence looks like. Parents with disabilities, like all parents, are creative and adaptable. In many cases, formal resources and supports are not available or accessible, and so some parents with disabilities may rely on unconventional resources and other supports to fulfill their roles effectively. At one time or another, everybody needs assistance whether they have a disability or not, and it is rare that someone really, truly raises a child single-handedly.
Moreover, for some mothers with physical disabilities, becoming a parent takes focus away from their disability and places it on other aspects of their lives, such as the new bond between parent and child as well as the child’s imagination and creativity. As Jane puts it, “Becoming a mom is probably the best thing that I did because it totally lessened … my focus or other people’s focus on my disability. My parents ask way less about my own health; they ask more about the kids.”
In particular, Jane talked about how her physical inability to do certain activities with her young son has led to opportunities to bond and play with him in other ways:
“[My son] knows that I do all the creative stuff with him, so I do all the artwork… he kind of sees us [my husband and me] as having those different [roles] … I love doing imaginative things and I think that’s important for his growing and learning … so for me what’s really boosted my confidence in parenting is that I have that ability or that gift to do that with him and the daycare has commented that he’s such a really imaginative kid…”
A number of other mothers who were interviewed shared similar stories about their relationships with their children and talked about how becoming a mother enhanced their confidence.
Many of the mothers also worried about how their children might be treated in school when other children found out that their mother has a disability: “Kids can be mean… I don’t want people to make fun of him because of me.” One mother with a congenital condition that often limits her mobility, as well as causes hearing and vision problems, arthritis and chronic pain, noted, however, that she uses her disability as a learning opportunity for her young son: “I don’t want him to make fun of anybody. I am trying to tell him that everyone is different.”
The experiences of women with physical disabilities during the perinatal period, including their parenting experiences, provide learning opportunities for all families and their children. This ongoing research project will help to develop resources for women with physical disabilities and health care providers and shed light on some of the positive experiences that they have during the perinatal period. Listening to and documenting the stories and experiences of women like Jane will be integral to this process of providing support.
Lesley A. Tarasoff is a Ph.D. candidate in Public Health at the University of Toronto. She conducts research in the area of women’s sexual and reproductive health, with a focus on women with physical disabilities and sexual minority women. For more information about her research, visit www.latarasoff.com.
Learn more:
Lesley A. Tarasoff, “We Don’t Know. We’ve Never had Anybody Like You Before”: Barriers to Perinatal care for Women with Physical Disabilities,” Disability and Health Journal 10:3 (July 2017). Link: http://bit.ly/2fmk65C.
Lori E. Ross, Lesley A. Tarasoff, Abbie E. Goldberg and Corey E. Flanders, “Pregnant Plurisexual Women’s Sexual and Relationship Histories Across the Life Span: A Qualitative Study,” Journal of Bisexuality (August 11, 2017). Link: http://bit.ly/2wfhZaN.
Lesley A. Tarasoff, “Experiences of Women with Physical Disabilities during the Perinatal Period: A Review of the Literature and Recommendations to Improve Care,” Health Care for Women International 36:1 (July 2013). Link: http://bit.ly/2hqbiQE.
Update: In September 2017, a community report was published based on this research into the experiences of women with physical disabilities. “Becoming Mothers: Experiences of Mothers with Physical Disabilities in Ontario” is now available to download on Lesley’s website.
SOURCES
Judith Rogers, The Disabled Woman’s Guide to Pregnancy and Birth (New York: Demos Medical Publishing, 2006).
Corbett Joan O’Toole, “Sex, Disability and Motherhood: Access to Sexuality for Disabled Mothers,” Disability Studies Quarterly 22:4 (2002).
Lisa I. Iezzoni, Jun Yu, Amy J. Wint, Suzanne C. Smeltzer and Jeffrey L. Ecker, “Prevalence of Current Pregnancy Among US Women with and without Chronic Physical Disabilities,” Medical Care, 51:6 (June 2013).
Alette Coble-Temple, Ayoka Bell and Kayoko Yokoyama, The Experience of Microaggressions on Women with Disabilities: From Research to Practice and Reproductive Microaggressions and Women with Physical Limitations. Presentations at the American Psychological Association Annual Convention (August 2014).
Derald Wing Sue, Jennifer Bucceri, Annie I. Lin, Kevin L. Nadal and Gina C. Torino, “Racial Microaggressions and the Asian American Experience,” Cultural Diversity and Ethnic Minority Psychology, 13:1 (2007).
Ayoka K. Bell, Nothing About Us Without Us: A Qualitative Investigation of the Experiences of Being a Target of Ableist Microaggressions (2013 doctoral dissertation), retrieved from ProQuest Dissertations and Theses (dissertation/thesis number 3620204).
Heather Kuttai, Maternity Rolls: Pregnancy, Childbirth and Disability (Fernwood Publishing, 2010).
Caroline Signore, Catherine Y. Spong, Danuta Krotoski, Nancy L. Shinowara and Sean Blackwell, “Pregnancy in Women with Physical Disabilities,” Obstetrics & Gynecology, 117:4 (2011).
Suzanne C. Smeltzer and Nancy C. Sharts-Hopko, A Provider’s Guide for the Care of Women with Physical Disabilities and Chronic Health Conditions (2005).
Published on December 3, 2015
Updated on September 25, 2017
Strength in Diversity: Positive Impacts of Children with Disabilities

Michelle R. Lodewyks
When it comes to exploring the experiences of families raising children with disabilities, studies tend to focus on the perceived negative impact of the disability on the family. These families are commonly viewed as “victims” who face excessive caregiving demands, emotional distress, physical and/or financial burdens and interpersonal difficulties, while the children are portrayed primarily as sources of stress and anguish. This tragedy dialogue supports an assumption that families with children with disabilities experience “chronic sorrow” and perpetuates the perception of disability as something to be avoided or eradicated. These perceptions have a major influence on today’s assumptions about – and reactions to – disability, including how professionals respond to children with disabilities and how society views and responds to children at birth. Consequently, the general public tends to overlook many positive impacts and meaningful contributions that children with disabilities make within their families, communities and society in general.
In order to explore the positive impact disability can have within families, a qualitative, interview-based study was performed to add narrative depth to the research. All of the parents and children interviewed identified a variety of positive effects the children have had on their families and contributions the children have made to family life. The most unsurprising discovery was the affirmation that a child with a disability can have some of the same positive effects on their families and make some of the same contributions as any other child. Highlighting these similarities is critical, given the tendency for children with disabilities to be distinguished from other children and viewed as less likely to affect their families in positive ways. Yet perhaps even more meaningful was the discovery that children with disabilities can also have unique positive effects and make unique contributions to families and family life.
Raising a child with a disability provides opportunities for personal growth
Parents in the study reported an ability to more readily recognize and appreciate the value, potential and strengths of a person with a disability as a result of their parenting experiences. Many described how their experiences left them with a greater acceptance of diversity, a stronger belief that there is an inherent and intrinsic value in people and a “more balanced appreciation for what people are about.”
One participant said her experience gave her a new perspective on how to help individuals she works with; she learned not to place limits on people or tell them what they can or cannot do, but instead help them strive for self-improvement. Siblings of children with a disability experienced attitudinal changes brought about by this family relationship. For these siblings, increased exposure to disability in their family environment made them more comfortable around other children with a disability, and they discovered a new-found enthusiasm for getting to know people with disabilities in general.
Children with a disability often exceeded expectations and did not necessarily comply with what is typical for their diagnoses, often being nothing close to the worst-case scenarios predicted by some doctors. As one participant stated, “I don’t know what my parents would have thought about people with disabilities before I came around, but I think it’s just… shown them that it really doesn’t mean that much… you can still be productive and still have goals and not really let anything stop you, as hard as that is sometimes.”
All of the parents in the study perceived themselves as having acquired new or enhanced positive character attributes as a result of raising a child with a disability. Attribute changes included family members learning to open their hearts and to be more loving, warm, caring, creative, balanced, gentle, calm, outgoing, responsible, independent and less selfish.
The positive attribute change most commonly reported by parents of a child with a disability was that they became more tolerant and accepting. As family members learned to be more accepting of diversity and of people’s behaviours, they cultivated a greater respect for other families of children with disabilities and experienced more compassion toward people in general.
Several parents commented that their child made them an overall “better person,” “better parent” or made other family members “better people.” Some of these effects carried over into the workplace: one participant perceived himself as a “better person at work” because of the understanding his son has given him about autism. This understanding has enabled him to relate to staff and other people in a different way; he supports his colleagues by helping them understand and interpret the behaviour of a co-worker who also has autism.
Parents experience pride, joy and strengthened relationships
All parents in the study reported positive emotions their children have fostered in them. A sense of pride was the most common. One parent recognized that some of the things that evoke a sense of pride “may not be the same as what other people [her son’s age] are doing,” yet she maintained she had numerous reasons to be proud. Parents expressed pride in, or were impressed by, their children’s knowledge or creativity, their sense of right and wrong, their methods for overcoming fears, their ability to put their minds to something and take a chance, and for being their own advocates. Additionally, all 10 children reported the positive emotions they also felt they evoked in family members – more than half believing they made their family proud.
One mother insisted she derives more excitement from the little things in life than many other people and that she “celebrate[s] things that other people don’t even think about celebrating” because of her daughter. Another explained her pride in her daughter as follows: “Disability-wise, I’m very proud of her because she hasn’t let her disability control her life. She’s got multiple disabilities… And she doesn’t let that slow her down… It would be too easy to say, ‘Oh, I can’t do this’ and give up… She’s always willing to push the limits and do the best that she can.”
Many parents talked about having met people, gained friendships and made new connections thanks to their child. While any child can expand a family’s social network, certain examples were attributed to the family’s particular circumstances. For one couple, connecting themselves to other families through the creation of a support network for parents with similar experiences has been valuable, as they have been able to offer support to other parents who have approached them for advice and guidance.
Despite one parent noting that having a child with a disability may make some families “fall apart,” many parents perceived that their child strengthened their marriage or made the parents and/or family stronger. Two of the parents felt they had become better at communicating and sharing with their spouse thanks to their child. The father in this couple talked about the difficulty he and his wife experienced when their son was first diagnosed and described the role each played in helping the other get through the “tough parts.” Their experience, he explained, has made him and his wife “more free to talk about things and feelings,” thus improving their communication.
A few parents mentioned how their child added a fresh perspective and/or insight to the family. One father commented on the value of his son’s insight and identified this as something he appreciates most about him: “His insight into things is so different than anybody else. He thinks differently than we do… and I love hearing his insight. He adds such a dimension to our house… I just can’t imagine not having that dimension in our home. It’s… such a core of who we are in this house. He’s so amazing.”
Referring to his natural gifts when it comes to writing and composing music, one of the children insisted that having autism has given him the ability to be hyperfocused and successful with music. He concluded, “I think the music is a positive impact. It can impact everyone else, too, if they hear it.”
When asked how she makes a difference in her family, another one of the children replied, “I suppose it would be a little less lively without me. There wouldn’t be as many interesting dinner conversations.” She also referred to “the whole yin and yang thing” and how she counterbalances the mellowness in her family.
Families learn from their unique experiences and seek to share their knowledge
Before concluding the interviews, all participants were asked what they would like other people to understand about them, their family and/or their experience. Parents shared that their experiences are “not all rosy” – that there have been “challenges,” “struggles,” “obstacles” and “tough times.” Yet parents did not necessarily hold the child responsible for any negative aspects of their experience. One parent admitted that her struggles adjusting to her child’s disability had less to do with the child than with other people’s preconceptions and the parents’ own feelings regarding what their experience would be like. She explained, “There was no question, that period of time where you struggle with it – a bit of a denial thing. Well, you almost grieve, but you come to the conclusion that those feelings are more about you, and what you thought, or what other people might be thinking.”
Other parents agreed that any anger, stress, anxiety and/or crises they may have experienced resulted from having to deal with the ignorance of other people and a general lack of societal understanding rather than from the child. One mother requested that people reconsider their use – or misuse – of certain labels, explaining that, while people with intellectual disabilities are often labelled as hindered in some way, “the hindrance is very often on the so-called ‘normal’ people for lack of understanding them.”
These findings coincided with those from an earlier study in which parents suggested that the sorrow they experienced originated largely from having to deal with recurring messages of negativity and hopelessness from other people, such as professionals, the health system, other family members and friends. This suggests a source of stress and negativity outside the child and that a family’s perceptions about their child may be determined, at least in part, by the surrounding cultural beliefs about disability. Therefore, if society holds negative attitudes toward disability and the surrounding cultural perceptions are largely negative, negativity can be transmitted to the family – to parents’ views of, and beliefs about, their children and to their parenting.
The parents in the study also wished to dispel negative assumptions others might associate with their child and place any negativity in context of the bigger picture. Some described their experience “as a gift instead of a burden,” and insisted it is not a source of anything negative to have a child with a disability in the family, emphasizing that they are not sorry for the way their child has changed their lives. While acknowledging the stress, hard work and commitment required to raise a child with a disability, other parents commented on the unfortunate nature of other people not realizing how rewarding the experience can be. One father reframed his experience raising his son in the following way: “You want a catastrophe? You want tragedy? You know what, let me pick up a paper and show you about somebody who died in a car accident. Let me show you about a young mother that was killed. Let me show you about the tsunami. Those are tragedies. This is a curveball. All you’ve got to do is learn how to hit curves and you’ll be fine… And it’s not easy, but you learn to grow with it.”
Among the most common requests from parents were that assumptions not be made based on disability and that people recognize each child’s ability and potential. Parents insisted that their children can give a lot to society and deserve respect and requested that people make an effort to learn from their children. Elaborating, one parent cautioned, “I was just thinking in terms of the impact of… people with Down syndrome on the world… We’ve been trying to basically eradicate this group of people by all the blood testing and stuff. It devalues the lives that they have. And they have something to offer… They’ve got something really special that we need to sit up and take note of because we could learn a lot from them.”
When asked what they wanted to share with others, similarly powerful messages came from the children. One of the children wanted others to “understand that I have disabilities, but I’m not a worse person for it.” Another child offered the following take-away message: “Lots of people have the perception that I’m kind of slow… I want them to know that I really do know a lot about the world and what’s going on, and it hasn’t stopped me – having cerebral palsy, being in a wheelchair – I’m not an unaware person. I have big ambitions and a bright future. I don’t want them to feel sorry for me, because I think I’m going to have a really good and interesting and fun life!”
The positivity of embracing diversity goes beyond the family
Learning from families who view their circumstances in a positive light, making these perceptions more readily available to the general public and coming to view the experience of raising a child with a disability as one that is not necessarily tragic – but rather enriching and rewarding – can have a variety of positive implications. These findings can provide medical professionals (particularly those involved in prenatal screening and diagnosis) with practical information to share with families when a diagnosis is given. These findings might also benefit other parents currently raising a child with a disability by encouraging them to focus more closely on what their child adds to their life.
In presenting these findings, this study is not denying the existence of challenges and negative family experiences. Sharing these findings is also not suggesting that everything will automatically improve for families who struggle raising a child with a disability. Yet the belief is that appreciating the strengths and positives has potential for beneficial change. There is also evidence that focusing on the children’s positive impacts and contributions may serve to control the meaning and level of stress associated with the experience. This could be helpful in the adaptation process. If more families see their experiences in a positive light, perhaps they can assist in altering widespread perceptions of the impact of disability, provide support to new parents and relieve some of the fear and anxiety around the idea of raising a child with a disability. In doing so, the hope is that a more affirmative way of viewing disability could be promoted.
Michelle Lodewyks is an Instructor in the Disability and Community Support Program at Red River College as well as a graduate of the Master’s Program in Disability Studies at the University of Manitoba.
SOURCES
Fotheringham, J. B., Skelton, M., & Hoddinott, B. (1971). The Retarded Child and His Family: The Effects of Home and Institution. Toronto, ON: Institute for Studies in Education.
Gupta, A., & Singhal, N. (2004). Positive Perceptions in Parents of Children with Disabilities. Asia Pacific Disability Rehabilitation Journal, 15:1. http://bit.ly/ZSm1oU (accessed October 9, 2014).
Kearney, P. M., & Griffin, T. (2001). Between Joy and Sorrow: Being a Parent of a Child with Developmental Disability. Journal of Advanced Nursing, 34:5.
Kharasch Behr, S. (1989). Underlying Dimensions of the Construct of Positive Contributions That Individuals with Developmental Disabilities Make to Their Families: A Factor Analytic Study. University of Kansas (unpublished doctoral dissertation).
Pearlin, L. I., & Schooler, C. (1978). The Structure of Coping. Journal of Health and Social Behavior, Vol. 19.
Stainton, T., & Besser, H. (1998). The Positive Impact of Children with an Intellectual Disability on the Family. Journal of Intellectual and Developmental Disability, 23:1. http://bit.ly/1s01wQt (accessed October 9, 2014).
Summers, J. A. (1988). Family Adjustment: Issues in Research on Families with Developmentally Disabled Children. In V. B. Van Hasselt, P. S. Strain and M. Hersen (Eds.), Handbook of Developmental and Physical Disabilities. Elmsford, NY: Pergamon.
Swain, J., & French, S. (2000). Towards an Affirmation Model of Disability. Disability & Society, 15:4. http://bit.ly/1ycgl7r (accessed October 9, 2014).
Whitney, D., & Trosten-Bloom, A. (2003). The Power of Appreciative Inquiry: A Practical Guide to Positive Change. San Francisco, CA: Berrett-Koehler Publishers, Inc.
Woolfson, L. (2003). Disabled Children, Parents and Society – A Need for Cognitive Reframing. Proceedings of the British Psychological Society, 11:1. http://bit.ly/1uGHSuW (accessed October 9, 2014).